
Tree Pollen Allergy Update
March 18, 2026 | Black & Kletz Allergy
 Well, it is this time of the year again. The time when pollen-allergic individuals are happy for the nicer weather, but often dread its consequences. For some, the relentless release of tree pollen causes a wide variety of annoying symptoms to occur, which is typical in the Spring in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Is also time for many individuals to seek care from a McLean allergist.
In the Washington DC area, trees begin to pollinate in February, reach a peak in April, and taper off in May, although some trees pollinate throughout the late Spring to the early Summer. Certain trees (e.g., maple, elm, juniper. alder) pollinate in the early Spring and certain trees (e.g. oak, birch, pine, sycamore) pollinate in the later Spring. One can always ask their McLean allergist for the exact timing of particular trees, if interested.
A question that many individuals living in the Washington, DC metropolitan area always ask is, what causes the yellowish coating of the cars that occurs every Spring? The answer is pine trees. It just so happens that pine tree pollen is very large in size and heavy, so it tends to land on surfaces. As a result, pine tree pollen is not very allergenic because it is too heavy to float in the air. Ironically however, oak tree pollen is highly allergenic and it is released at the same time pine tree pollen is released. Unlike pine tree pollen, oak tree pollen is small in size which allows the pollen grains to enter the nose and sinuses easily, triggering immune and allergic reactions. Oak tree pollen is one of the main culprits for causing allergies in our area. In fact, oak trees are the major tree in our area that seems to produce the most amount of allergic symptoms in patients. The Washington area has millions of oak trees in its forests and neighborhoods. They are one of the dominant native trees in the Mid-Atlantic region. When the pine trees release pollen all at once, it creates that famous yellow Spring haze, but the pine tree pollen is generally not causing allergic symptoms in most of the allergy sufferers. Simultaneously however, the oak trees are also releasing their pollen which does bother tree pollen-sensitive individuals causing them to have the classic hay fever (i.e., allergic rhinitis) symptoms. To put this in perspective, a single large oak tree can release billions of pollen grains in one season. This fact gives an insight as to why so many people at this time of year seek a McLean allergist to help relieve these bothersome symptoms that result from exposure to tree pollens in allergic individuals.
Washington, DC tends to have more tree pollen than many cities in the United States. This occurs for several different reasons. The Mid-Atlantic originally had dense oak–hickory forests. Even today, much of the area around DC (i.e., Maryland and Northern Virginia) still has large tree coverage. The major tree pollens (e.g., maple, hickory, sycamore, birch, oak) are wind-pollinated, which means they release a lot of pollen into the air. In fact, Washington was designed with large green spaces and tree-lined streets. The parks (i.e., Rock Creek Park, National Mall, and Arboretum) plus the neighborhood trees create a huge urban canopy. Roughly 35–40% of the city is covered by tree canopy, which is very high for a major city. It is thus understandable that many tree pollen-sensitive individuals often look for a McLean allergist in the Spring in order to diagnose and treat the unwanted symptoms that result from being exposed to so much tree pollen.
In addition to the numerous trees in Washington, DC, landscapers in the 20th century preferred male trees because they do not produce fruit or seeds that could fall on the sidewalks of the nation’s capital. The problem is that male trees produce all the pollen. While being a good choice for the aesthetics of the city, it unfortunately was not a good decision for tree pollen-allergic individuals. Also, Washington, DC’s warm and early Springs, windy days, and dry periods all tend to be the perfect combination of factors or the “perfect storm” to produce very intense pollen seasons.
The characteristic allergic symptoms experienced by allergy sufferers may include sneezing, runny nose, nasal congestion, post-nasal drip, itchy nose, itchy throat, sinus headaches, snoring, itchy eyes, watery eyes, and/or redness of the eyes. Individuals with asthma may develop a worsening of their asthma. These individuals may complain of chest tightness, wheezing, coughing, and/or shortness of breath. Patients with moderate to severe signs or symptoms of the pollen allergies should see a McLean allergist for diagnosis and treatment.
The diagnosis of allergic rhinitis (i.e., hay fever) and/or allergic conjunctivitis (i.e., eye allergies) begins with the McLean allergist obtaining a comprehensive history and physical examination. Allergy skin testing, and/or occasionally allergy blood testing, is usually performed in order to determine if and how allergic a patient is to a specific aeroallergen. A board certified McLean allergist would be the person to see if one lives in the vicinity. If our McLean office is not convenient, Black & Kletz Allergy has another office locations on K Street in Washington, DC, as well as an office in Manassas, VA.
The treatment of allergic rhinitis and allergic conjunctivitis mainly consists of avoiding the allergen, if possible and using medications designed to treat allergies. Medications may include antihistamines, decongestants, leukotriene antagonists, nasal corticosteroids, nasal antihistamines, nasal anticholinergics, nasal mast cell stabilizers, ocular antihistamines, and/or ocular mast cell stabilizers. In addition to medications, allergy immunotherapy (i.e., allergy shots, allergy injections, allergy desensitization, allergy hyposensitization) is very efficacious. It typically helps about 80-85% of individuals who take them. The average length of time on allergy immunotherapy is approximately 3-5 years. Seeing a board certified McLean allergist like the ones at Black & Kletz Allergy may be beneficial because they can diagnose and treat these maddening allergy symptoms in order for you to have a better quality of life.
The board certified allergists at Black & Kletz Allergy will promptly answer any questions you may have regarding tree pollen allergies and asthma. Our allergists have been diagnosing and treating seasonal allergies as well as all other types of allergies in the Washington, DC, Northern Virginia, and Maryland metropolitan area for more than 50 years. We have 3 convenient locations in the DC metro area with offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. There is on-site parking at each location and both the Washington, DC and McLean, VA offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call us at any one of our 3 locations. Alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy is dedicated in providing the most up-to-date diagnostic and treatment modalities in the field of allergy, asthma, and immunology.
Well, it is this time of the year again. The time when pollen-allergic individuals are happy for the nicer weather, but often dread its consequences. For some, the relentless release of tree pollen causes a wide variety of annoying symptoms to occur, which is typical in the Spring in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Is also time for many individuals to seek care from a McLean allergist.
In the Washington DC area, trees begin to pollinate in February, reach a peak in April, and taper off in May, although some trees pollinate throughout the late Spring to the early Summer. Certain trees (e.g., maple, elm, juniper. alder) pollinate in the early Spring and certain trees (e.g. oak, birch, pine, sycamore) pollinate in the later Spring. One can always ask their McLean allergist for the exact timing of particular trees, if interested.
A question that many individuals living in the Washington, DC metropolitan area always ask is, what causes the yellowish coating of the cars that occurs every Spring? The answer is pine trees. It just so happens that pine tree pollen is very large in size and heavy, so it tends to land on surfaces. As a result, pine tree pollen is not very allergenic because it is too heavy to float in the air. Ironically however, oak tree pollen is highly allergenic and it is released at the same time pine tree pollen is released. Unlike pine tree pollen, oak tree pollen is small in size which allows the pollen grains to enter the nose and sinuses easily, triggering immune and allergic reactions. Oak tree pollen is one of the main culprits for causing allergies in our area. In fact, oak trees are the major tree in our area that seems to produce the most amount of allergic symptoms in patients. The Washington area has millions of oak trees in its forests and neighborhoods. They are one of the dominant native trees in the Mid-Atlantic region. When the pine trees release pollen all at once, it creates that famous yellow Spring haze, but the pine tree pollen is generally not causing allergic symptoms in most of the allergy sufferers. Simultaneously however, the oak trees are also releasing their pollen which does bother tree pollen-sensitive individuals causing them to have the classic hay fever (i.e., allergic rhinitis) symptoms. To put this in perspective, a single large oak tree can release billions of pollen grains in one season. This fact gives an insight as to why so many people at this time of year seek a McLean allergist to help relieve these bothersome symptoms that result from exposure to tree pollens in allergic individuals.
Washington, DC tends to have more tree pollen than many cities in the United States. This occurs for several different reasons. The Mid-Atlantic originally had dense oak–hickory forests. Even today, much of the area around DC (i.e., Maryland and Northern Virginia) still has large tree coverage. The major tree pollens (e.g., maple, hickory, sycamore, birch, oak) are wind-pollinated, which means they release a lot of pollen into the air. In fact, Washington was designed with large green spaces and tree-lined streets. The parks (i.e., Rock Creek Park, National Mall, and Arboretum) plus the neighborhood trees create a huge urban canopy. Roughly 35–40% of the city is covered by tree canopy, which is very high for a major city. It is thus understandable that many tree pollen-sensitive individuals often look for a McLean allergist in the Spring in order to diagnose and treat the unwanted symptoms that result from being exposed to so much tree pollen.
In addition to the numerous trees in Washington, DC, landscapers in the 20th century preferred male trees because they do not produce fruit or seeds that could fall on the sidewalks of the nation’s capital. The problem is that male trees produce all the pollen. While being a good choice for the aesthetics of the city, it unfortunately was not a good decision for tree pollen-allergic individuals. Also, Washington, DC’s warm and early Springs, windy days, and dry periods all tend to be the perfect combination of factors or the “perfect storm” to produce very intense pollen seasons.
The characteristic allergic symptoms experienced by allergy sufferers may include sneezing, runny nose, nasal congestion, post-nasal drip, itchy nose, itchy throat, sinus headaches, snoring, itchy eyes, watery eyes, and/or redness of the eyes. Individuals with asthma may develop a worsening of their asthma. These individuals may complain of chest tightness, wheezing, coughing, and/or shortness of breath. Patients with moderate to severe signs or symptoms of the pollen allergies should see a McLean allergist for diagnosis and treatment.
The diagnosis of allergic rhinitis (i.e., hay fever) and/or allergic conjunctivitis (i.e., eye allergies) begins with the McLean allergist obtaining a comprehensive history and physical examination. Allergy skin testing, and/or occasionally allergy blood testing, is usually performed in order to determine if and how allergic a patient is to a specific aeroallergen. A board certified McLean allergist would be the person to see if one lives in the vicinity. If our McLean office is not convenient, Black & Kletz Allergy has another office locations on K Street in Washington, DC, as well as an office in Manassas, VA.
The treatment of allergic rhinitis and allergic conjunctivitis mainly consists of avoiding the allergen, if possible and using medications designed to treat allergies. Medications may include antihistamines, decongestants, leukotriene antagonists, nasal corticosteroids, nasal antihistamines, nasal anticholinergics, nasal mast cell stabilizers, ocular antihistamines, and/or ocular mast cell stabilizers. In addition to medications, allergy immunotherapy (i.e., allergy shots, allergy injections, allergy desensitization, allergy hyposensitization) is very efficacious. It typically helps about 80-85% of individuals who take them. The average length of time on allergy immunotherapy is approximately 3-5 years. Seeing a board certified McLean allergist like the ones at Black & Kletz Allergy may be beneficial because they can diagnose and treat these maddening allergy symptoms in order for you to have a better quality of life.
The board certified allergists at Black & Kletz Allergy will promptly answer any questions you may have regarding tree pollen allergies and asthma. Our allergists have been diagnosing and treating seasonal allergies as well as all other types of allergies in the Washington, DC, Northern Virginia, and Maryland metropolitan area for more than 50 years. We have 3 convenient locations in the DC metro area with offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. There is on-site parking at each location and both the Washington, DC and McLean, VA offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call us at any one of our 3 locations. Alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy is dedicated in providing the most up-to-date diagnostic and treatment modalities in the field of allergy, asthma, and immunology.
Chronic Rhinosinusitis With Nasal Polyps
March 10, 2026 | Black & Kletz Allergy
 Chronic rhinosinusitis (i.e., long-standing inflammation of the tissues inside the nasal cavity and sinuses inside the facial bones) is one of the most common medical conditions, affecting approximately 12% of the population. In roughly 20% of these patients, there is an association with nasal polyps and the condition is thus named “chronic rhinosinusitis with nasal polyps.”
Nasal polyps are soft tissue growths that form on the lining of the nasal passages and inside the sinuses (i.e., air-filled cavities within the facial bones). Nasal polyps are painless and non-cancerous. They are usually in the shape of teardrops and glisten like moist grapes. Polyps develop when the mucus membranes are chronically inflamed and swell up over a long period of time.
When the polyps grow large, they can obstruct the nasal passages and cause breathing difficulties. They can also block the free passage of secretions from the sinuses into the nose. This blockage predisposes individuals with nasal polyps to sinus infections.
Any condition which results in chronic inflammation inside the nose and sinuses may lead to polyp formation. Some of these conditions are as follows:
Chronic rhinosinusitis (i.e., long-standing inflammation of the tissues inside the nasal cavity and sinuses inside the facial bones) is one of the most common medical conditions, affecting approximately 12% of the population. In roughly 20% of these patients, there is an association with nasal polyps and the condition is thus named “chronic rhinosinusitis with nasal polyps.”
Nasal polyps are soft tissue growths that form on the lining of the nasal passages and inside the sinuses (i.e., air-filled cavities within the facial bones). Nasal polyps are painless and non-cancerous. They are usually in the shape of teardrops and glisten like moist grapes. Polyps develop when the mucus membranes are chronically inflamed and swell up over a long period of time.
When the polyps grow large, they can obstruct the nasal passages and cause breathing difficulties. They can also block the free passage of secretions from the sinuses into the nose. This blockage predisposes individuals with nasal polyps to sinus infections.
Any condition which results in chronic inflammation inside the nose and sinuses may lead to polyp formation. Some of these conditions are as follows:
- Allergic rhinitis
- Chronic sinusitis
- Aspirin sensitivity
- Asthma
- Cystic fibrosis
- Eosinophilic disorders
- Allergic fungal sinusitis
- Nasal congestion
- Runny nose
- Post-nasal drip
- Diminished sense of taste and smell
- Facial pressure/headaches
- Snoring
- Endoscopic examination of nose
- Imaging studies such as Xrays and CT scans
- Allergy tests
- Sweat chloride test for cystic fibrosis
- Eosinophil count in the peripheral blood
- Measurement of biomarkers such as periostin
- Long-term (i.e., chronic sinusitis) or repeated sinus infections
- Nosebleeds (i.e., epistaxis)
- Asthma exacerbations
- Obstructive sleep apnea
- Double vision (i.e., diplopia)
Post-Nasal Drip
February 11, 2026 | Black & Kletz Allergy
 A common complaint among patients is the need to clear their throats frequently in an attempt to get relief from a feeling of “irritation” in their throats. This feeling is often termed “post-nasal drip,” implying excessive secretions from the upper respiratory tract draining down the back of the throat.
All because the feeling of a post-nasal drip is present, there are many other conditions or processes that may result in the sensation of throat irritation. Post-nasal drip is primarily a subjective complaint with no definitive objective diagnostic criteria.
It should be pointed out that a chronic cough is one of the most bothersome symptoms triggered by a post-nasal drip, however, hoarseness, bad breath, and sore throat are other common manifestations of a post-nasal drip.
There are many conditions that predispose an individual to a post-nasal drip and some of them are listed below:
A common complaint among patients is the need to clear their throats frequently in an attempt to get relief from a feeling of “irritation” in their throats. This feeling is often termed “post-nasal drip,” implying excessive secretions from the upper respiratory tract draining down the back of the throat.
All because the feeling of a post-nasal drip is present, there are many other conditions or processes that may result in the sensation of throat irritation. Post-nasal drip is primarily a subjective complaint with no definitive objective diagnostic criteria.
It should be pointed out that a chronic cough is one of the most bothersome symptoms triggered by a post-nasal drip, however, hoarseness, bad breath, and sore throat are other common manifestations of a post-nasal drip.
There are many conditions that predispose an individual to a post-nasal drip and some of them are listed below:
- Allergic rhinitis (Hay fever): The inflamed nasal mucus membranes secrete excessive mucus in patients with allergies.
- Non-allergic rhinitis: Some examples of this condition include gustatory rhinitis (i.e., related to eating where eating any food may trigger a runny nose or post-nasal drip), neurologic rhinitis, and rhinitis caused by other irritants such as smoke, strong scents (e.g., perfumes, cleaning solutions), changes in barometric pressure, changes in temperatures).
- Nasal polyps: The increased surface area of the mucus membranes from excessive tissue growth of the nasal polyp results in oversecretion of mucus.
- Ciliary dyskinesia: Dysfunction or reduced activity of the ciliary (hair-like) structures which promote normal drainage of secretions.
- Cystic fibrosis: A genetically determined condition which causes abundant thick mucus production.
- Heightened body awareness or hypersensitivity
- Upper respiratory tract infections: May cause ciliary damage and thus prolonged symptoms.
- Chronic rhinosinusitis: Typically caused by viral, bacterial, or fungal infections.
- Laryngopharyngeal reflux (LPR): Gastroesophageal reflux disease (GERD)-related disorder usually resulting in a sore throat and/or hoarseness.
- Comprehensive history and physical examination
- Allergy skin testing or allergy blood testing
- Rhinoscopy: A direct visualization procedure of the tissues in the nose and the back of the throat that can be done in the office. It is when the physician puts a thin long tube up one’s nose in order to look in the nose, throat, and vocal cords. Rhinoscopy identifies posterior nasal secretions but has a limited sensitivity and specificity. Patient-reported frequency and severity of symptoms do not always correlate with the abnormalities detected by rhinoscopy.
- Fluorescent particle tracking: May show slower mucociliary clearance and more viscous mucus.
- The Sinonasal Outcome Test (SNOT) is used to measure symptom severity. It is a subjective 0-5 scale where patients report bothersome symptoms, including postnasal drip.
- Associated symptoms may include nasal congestion, poor sense of smell and taste, facial pressure, and/or difficulty in sleeping
- Chronic rhinosinusitis: Functional endoscopic sinus surgery, posterior nasal nerve ablation, etc.
- Allergic rhinitis: Antihistamine (e.g., azelastine, olopatadine), corticosteroid (e.g., fluticasone, mometasone, budesonide), and anticholinergic (e.g., ipratropium bromide) nasal sprays, oral antihistamines (e.g., loratadine, desloratadine, fexofenadine, cetirizine, levocetirizine), and/or allergen immunotherapy (i.e., allergy shots, allergy injections, allergy desensitization, allergy hyposensitization) to environmental allergens. Allergy shots are effective in 80-85% of patients. The average length allergy immunotherapy treatment is typically 3-5 years.
- A humidifier or steam inhalation (as occurs in a hot shower)
- Keeping well-hydrated: Keeps the mucus thinner.
- Sleep on propped up pillows, to keep the mucus from collecting at the back of the throat
- Nasal irrigation: Available over-the-counter saline preparations
- Oral decongestant: Such as pseudoephedrine (e.g., Sudafed)
- Mucolytic agents: Medications that thin out mucus such as Guaifenesin (e.g., Mucinex)
- Gastroesophageal reflux disease (GERD): Lifestyle modifications may help to reduce acid secretion. Proton pump inhibitors (e.g., pantoprazole, omeprazole, esomeprazole, lansoprazole, rabeprazole, dexlansoprazole) may help alleviate symptoms.
- Biologics: Medications such as omalizumab (i.e., Xolair) and dupilumab (i.e., Dupixent) show moderate efficacy.
Update on Mast Cell Activation Syndrome (MCAS)
February 3, 2026 | Black & Kletz Allergy
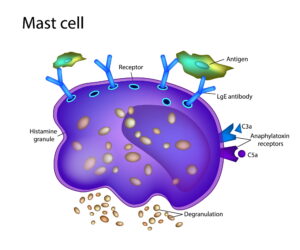 Mast cell activation syndrome (MCAS) is caused by episodic abnormal release of chemical mediators stored in the granules of mast cells which may affect any organ system. The organ systems most affected tend to involve the skin, gastrointestinal tract, nervous system, and cardiovascular system primarily. Although the prevalence of mast cell activation syndrome varies a lot depending on the source, it is pretty clear that the prevalence has been increasing over recent 5-10 years, particularly since the coronavirus pandemic. The syndrome tends to affect women more than men.
What is a mast cell?
A mast cell is a type of specialized white blood cell that serves as the “alarm system” for the immune system. Unlike normal white blood cells which circulate in the bloodstream, mast cells are found in the connective tissues of the body, especially in areas that interface with the external environment, such as the skin, gastrointestinal tract, and lungs. Mast cells use their receptors on their surface to detect “intruders” such as allergens, bacteria, viruses, and/or parasites. When a mast cell notices a threat, it "degranulates,” a procedure where it quickly bursts open hundreds of tiny sacs (i.e., granules) which in turn releases chemical mediators that were stored in those granules. As a result, chemical mediators (i.e., histamine, heparin, tryptase, cytokines) signal other immune cells to rush to the area. They cause blood vessels to expand, leading to flushing and swelling, as well as muscles to contract, causing coughing or gastrointestinal tract symptoms, in order to help flush out the threat.
What does each chemical mediator do?
As mentioned above, the key chemical mediators released from mast cells and their primary effect are as follows:
Mast cell activation syndrome (MCAS) is caused by episodic abnormal release of chemical mediators stored in the granules of mast cells which may affect any organ system. The organ systems most affected tend to involve the skin, gastrointestinal tract, nervous system, and cardiovascular system primarily. Although the prevalence of mast cell activation syndrome varies a lot depending on the source, it is pretty clear that the prevalence has been increasing over recent 5-10 years, particularly since the coronavirus pandemic. The syndrome tends to affect women more than men.
What is a mast cell?
A mast cell is a type of specialized white blood cell that serves as the “alarm system” for the immune system. Unlike normal white blood cells which circulate in the bloodstream, mast cells are found in the connective tissues of the body, especially in areas that interface with the external environment, such as the skin, gastrointestinal tract, and lungs. Mast cells use their receptors on their surface to detect “intruders” such as allergens, bacteria, viruses, and/or parasites. When a mast cell notices a threat, it "degranulates,” a procedure where it quickly bursts open hundreds of tiny sacs (i.e., granules) which in turn releases chemical mediators that were stored in those granules. As a result, chemical mediators (i.e., histamine, heparin, tryptase, cytokines) signal other immune cells to rush to the area. They cause blood vessels to expand, leading to flushing and swelling, as well as muscles to contract, causing coughing or gastrointestinal tract symptoms, in order to help flush out the threat.
What does each chemical mediator do?
As mentioned above, the key chemical mediators released from mast cells and their primary effect are as follows:
- Histamine - Increases blood flow and causes itching, swelling, and mucus production.
- Heparin - Prevents blood clotting to keep blood flowing to the affected area.
- Tryptase - An enzyme used as a marker for mast cell activity; It helps break down tissue to allow immune cells to move.
- Cytokines - Small proteins that recruit other immune cells and signal the body to create more white blood cells.
- Emotional and Physical Stress – Emotional trauma or anxiety and physical stressors such as pain, major surgery, and/or lack of sleep.
- Environmental Factors – Extreme heat, extreme cold, sudden changes in temperature, high humidity, and/or sunlight.
- Food and Drink – High histamine foods: Alcohol (especially beer and red wine), fermented foods (e.g., aged cheeses, soy sauce, sauerkraut, kombucha), chocolate, tomatoes, citrus fruits, pineapples, kiwi, bananas, strawberries, papayas, plums, spinach, eggplant, peanuts, walnuts, cashews, chickpeas, cured meats, food additives (e.g., MSG, artificial dyes), ketchup, mustard, and/or shellfish
- Odors and Chemicals - Fragrances (i.e., perfumes, colognes), cigarette smoke, cleaning supplies, pesticides, and/or "new car" or "new carpet" smells.
- Physical Stimuli - Friction or vibration on the skin (i.e., rubbing, tight clothing), and/or intense exercise.
- Hormonal Changes - Fluctuations in estrogen levels (i.e., estrogen treatment, menstruation, pregnancy, menopause)
- Infections - Bacterial, viral, or fungal infections (e.g., COVID-19, influenza, strep. infection).
- Insect Bites/Stings - Venom from bee, wasp, yellow jacket, hornet, and/or fire ant stings
- Medications - Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (e.g., Motrin, Advil), naproxen (e.g., Aleve, Naprosyn), opioids (e.g., codeine, morphine), aspirin, certain antibiotics, and/or contrast dyes used in medical imaging (e.g., IV radiocontrast dye)
Asthma in the Winter Updated 2026
January 22, 2026 | Black & Kletz Allergy
 It is Winter in the Washington, DC, Northern, VA, and Maryland metropolitan area which generally means cold and dry weather. Individuals with asthma may be affected more than the usual person during the Winter because the cold weather is a common trigger of asthma. An asthma doctor DC residents trust is important to the health of anyone in the metro area with asthma. At Black & Kletz Allergy, we have asthma doctors DC locals have used for decades to help them with their treatment of allergies and asthma.
In addition to cold air, upper respiratory tract infections (URIs) are a very common asthma trigger in many asthmatics. The infectious agents can be viral, bacterial, or fungal in origin. During the Winter months, it is extremely common to be exposed to a variety of infections. Viruses such as influenza (i.e., flu), respiratory syncytial virus (RSV), COVID-19, rhinovirus, adenovirus, human metapneumovirus (hMPV), and parainfluenza are fairly prevalent. Interestingly, it is not the cold weather that makes individuals more susceptible to these viruses. Instead, when it is cold outside, people tend to spend more time indoors with each other, and as a result, the close proximity to other individuals allows for easier transmission of viruses from one person to another.
Upper respiratory viruses cause airway inflammation, increased mucus production, and constriction of the bronchial tubes which usually leads to an exacerbation of an individual’s asthma symptoms. The classic symptoms that result are wheezing, chest tightness, coughing, and/or shortness of breath. In many asthma patients, pneumonia may occur. An asthma doctor DC inhabitants trust, such as the board certified allergists at Black & Kletz Allergy, should be notified when a patient has an exacerbation of one’s asthma. It should be noted that asthmatic airways are already inflamed and sensitive, making them more prone to swelling. Upper respiratory infections with viruses such as rhinovirus RSV, influenza, parainfluenza, adenovirus, human metapneumovirus or coronavirus can damage the airway lining, trigger immune responses, and/or worsen bronchial hyperresponsiveness, resulting in breathing difficulties and requiring more short-acting, quick-relief asthma rescue medication such as albuterol (e.g., Proventil, Ventolin, ProAir), levalbuterol (e.g., Xopenex), or albuterol/budesonide (e.g., AirSupra).
Certain environmental allergens also play an important role in how bothersome someone’s asthma may be. During the Winters in the DC metro area, indoor allergens (i.e., dust mites, molds, pets, cockroach) and some outdoor allergens (i.e., molds) are common aggravators of asthma. Individuals that are sensitive to these environmental allergens may experience worsening of their asthma and/or allergic rhinitis (i.e., hay fever) symptoms.
Dust mites tend to be an important trigger, particularly to inner city children. The dust mites are typically found in bedding (e.g., pillows, mattresses, box springs), carpeting, and upholstered furniture to name a few. It is advisable for patients to cover their bedroom pillows, mattress, and box spring with allergy-proof encasings. These encasings usually zip up over the pillows, mattress, and box spring. An asthma doctor DC residents admire will help the patient avoid dust mites with different options.
Unlike dust mites, mold is found both indoors and outdoors. Mold is ubiquitous and may trigger an asthma exacerbation in mold-sensitive individuals. In buildings, mold typically is found in moist and damp areas such as bathrooms, kitchens, and basements. Using a dehumidifier may help reduce the amount of mold present inside one’s home. Molds that are outdoors are more difficult to control, however, avoiding mowing the lawn, raking the leaves, and other activities where mold exposure is high are recommended. Again, an allergy or asthma doctor DC locals find helpful will steer one in the right direction.
Pets’ saliva and dander are found mostly indoors, and they may be a significant trigger to someone’s asthma. Pet allergies tend to be worse during the Winter because people’s homes tend to be closed up more during this time causing the pet allergen to be more prevalent. It is prudent to avoid direct contact with a pet if the person is sensitive to that type of pet. Touching one’s eyes may cause itching, watery, puffiness, and/or redness of the eyes in pet-allergic individuals. An asthma doctor DC residents trust would also advise for that person to avoid having that pet go in their bedroom, so there is a “safe” space in their home.
Cockroaches are also mostly an indoor allergen. Cockroach allergies are quite common in big cities, such as Washington, D.C. Many homes, condos, apartments, public buildings, and restaurants in inner cities are infested with cockroaches, even though they may not be visible during the day to most people. It is vital to make sure that traces of food are not left on floors and counters, as this invites cockroaches. There is also a clear association between cockroach allergy and childhood asthma in inner city populations. In addition to asthma, cockroach allergies may cause allergic rhinitis (i.e., hay fever) and/or allergic conjunctivitis (i.e., eye allergies) in sensitive allergic individuals. An allergy or asthma doctor DC inhabitants have confidence in will recommend being as clean as possible to try to avoid having cockroaches in one’s home.
Other than avoiding all the allergens mentioned above that are common during the Winter, there are various medications that can be utilized by allergy and asthma doctors DC locals trust to treat dust mites, mold, pet, and cockroach allergies. In addition to various antihistamines, decongestants, nasal sprays, and allergy eye drops, allergy shots (i.e., allergy injections, allergy immunotherapy, allergy desensitization) are a very effective tool that board certified allergists use to treat people with these allergies. Allergy shots are efficacious in 80-85% of the individuals that take them. Allergy immunotherapy has been used in the U.S. to treat asthma and allergies for more than a century. The typical length of therapy is 3-5 years.
The board certified allergy doctors at Black & Kletz Allergy have been diagnosing and treating asthma and allergies for more than 50 years in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Our offices are conveniently located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. Each office has on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and there is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. Please call for an appointment if you would like a consultation with one of our allergists, or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy prides itself in providing quality allergy and asthma care to the Washington, DC metropolitan area community.
It is Winter in the Washington, DC, Northern, VA, and Maryland metropolitan area which generally means cold and dry weather. Individuals with asthma may be affected more than the usual person during the Winter because the cold weather is a common trigger of asthma. An asthma doctor DC residents trust is important to the health of anyone in the metro area with asthma. At Black & Kletz Allergy, we have asthma doctors DC locals have used for decades to help them with their treatment of allergies and asthma.
In addition to cold air, upper respiratory tract infections (URIs) are a very common asthma trigger in many asthmatics. The infectious agents can be viral, bacterial, or fungal in origin. During the Winter months, it is extremely common to be exposed to a variety of infections. Viruses such as influenza (i.e., flu), respiratory syncytial virus (RSV), COVID-19, rhinovirus, adenovirus, human metapneumovirus (hMPV), and parainfluenza are fairly prevalent. Interestingly, it is not the cold weather that makes individuals more susceptible to these viruses. Instead, when it is cold outside, people tend to spend more time indoors with each other, and as a result, the close proximity to other individuals allows for easier transmission of viruses from one person to another.
Upper respiratory viruses cause airway inflammation, increased mucus production, and constriction of the bronchial tubes which usually leads to an exacerbation of an individual’s asthma symptoms. The classic symptoms that result are wheezing, chest tightness, coughing, and/or shortness of breath. In many asthma patients, pneumonia may occur. An asthma doctor DC inhabitants trust, such as the board certified allergists at Black & Kletz Allergy, should be notified when a patient has an exacerbation of one’s asthma. It should be noted that asthmatic airways are already inflamed and sensitive, making them more prone to swelling. Upper respiratory infections with viruses such as rhinovirus RSV, influenza, parainfluenza, adenovirus, human metapneumovirus or coronavirus can damage the airway lining, trigger immune responses, and/or worsen bronchial hyperresponsiveness, resulting in breathing difficulties and requiring more short-acting, quick-relief asthma rescue medication such as albuterol (e.g., Proventil, Ventolin, ProAir), levalbuterol (e.g., Xopenex), or albuterol/budesonide (e.g., AirSupra).
Certain environmental allergens also play an important role in how bothersome someone’s asthma may be. During the Winters in the DC metro area, indoor allergens (i.e., dust mites, molds, pets, cockroach) and some outdoor allergens (i.e., molds) are common aggravators of asthma. Individuals that are sensitive to these environmental allergens may experience worsening of their asthma and/or allergic rhinitis (i.e., hay fever) symptoms.
Dust mites tend to be an important trigger, particularly to inner city children. The dust mites are typically found in bedding (e.g., pillows, mattresses, box springs), carpeting, and upholstered furniture to name a few. It is advisable for patients to cover their bedroom pillows, mattress, and box spring with allergy-proof encasings. These encasings usually zip up over the pillows, mattress, and box spring. An asthma doctor DC residents admire will help the patient avoid dust mites with different options.
Unlike dust mites, mold is found both indoors and outdoors. Mold is ubiquitous and may trigger an asthma exacerbation in mold-sensitive individuals. In buildings, mold typically is found in moist and damp areas such as bathrooms, kitchens, and basements. Using a dehumidifier may help reduce the amount of mold present inside one’s home. Molds that are outdoors are more difficult to control, however, avoiding mowing the lawn, raking the leaves, and other activities where mold exposure is high are recommended. Again, an allergy or asthma doctor DC locals find helpful will steer one in the right direction.
Pets’ saliva and dander are found mostly indoors, and they may be a significant trigger to someone’s asthma. Pet allergies tend to be worse during the Winter because people’s homes tend to be closed up more during this time causing the pet allergen to be more prevalent. It is prudent to avoid direct contact with a pet if the person is sensitive to that type of pet. Touching one’s eyes may cause itching, watery, puffiness, and/or redness of the eyes in pet-allergic individuals. An asthma doctor DC residents trust would also advise for that person to avoid having that pet go in their bedroom, so there is a “safe” space in their home.
Cockroaches are also mostly an indoor allergen. Cockroach allergies are quite common in big cities, such as Washington, D.C. Many homes, condos, apartments, public buildings, and restaurants in inner cities are infested with cockroaches, even though they may not be visible during the day to most people. It is vital to make sure that traces of food are not left on floors and counters, as this invites cockroaches. There is also a clear association between cockroach allergy and childhood asthma in inner city populations. In addition to asthma, cockroach allergies may cause allergic rhinitis (i.e., hay fever) and/or allergic conjunctivitis (i.e., eye allergies) in sensitive allergic individuals. An allergy or asthma doctor DC inhabitants have confidence in will recommend being as clean as possible to try to avoid having cockroaches in one’s home.
Other than avoiding all the allergens mentioned above that are common during the Winter, there are various medications that can be utilized by allergy and asthma doctors DC locals trust to treat dust mites, mold, pet, and cockroach allergies. In addition to various antihistamines, decongestants, nasal sprays, and allergy eye drops, allergy shots (i.e., allergy injections, allergy immunotherapy, allergy desensitization) are a very effective tool that board certified allergists use to treat people with these allergies. Allergy shots are efficacious in 80-85% of the individuals that take them. Allergy immunotherapy has been used in the U.S. to treat asthma and allergies for more than a century. The typical length of therapy is 3-5 years.
The board certified allergy doctors at Black & Kletz Allergy have been diagnosing and treating asthma and allergies for more than 50 years in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Our offices are conveniently located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. Each office has on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and there is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. Please call for an appointment if you would like a consultation with one of our allergists, or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy prides itself in providing quality allergy and asthma care to the Washington, DC metropolitan area community.
Update on Alpha-Gal Syndrome
January 16, 2026 | Black & Kletz Allergy
 Alpha-gal syndrome is an allergic condition caused by a sensitivity to a carbohydrate known as galactose-alpha-1,3-galactose (i.e., alpha-gal). This molecule is found on the cells of non-primate mammals (i.e., beef, pork, lamb, venison, etc.). This condition is mainly thought to develop after tick bites. The regional distribution of alpha-gal syndrome corresponds with specific tick species populations (e.g., the lone star tick). Alpha-gal syndrome is also called mammalian meat allergy.
In the United States, the prevalence of lone start ticks and alpha-gal syndrome is highest in the Southeast region. Overall, the prevalence of alpha-gal syndrome is thought to be rising, with current estimates suggesting that up to 450,000 cases have occurred in the U.S. since 2010. It was first diagnosed in Virginia.
Other organisms besides ticks have been implicated in the potential induction of alpha-gal sensitization and clinical reactivity. One study demonstrated a correlation between alpha-gal-specific IgE antibody levels and exposure to an intestinal parasite called Ascaris lumbricoides (i.e., round worm). Moreover, some data suggest that bee and wasp stings may also contribute to the production of alpha-gal-specific IgE, particularly in beekeeping populations.
Besides muscle and organ meats, dairy products have also been implicated in triggering reactions. Additionally, gelatin, (commonly derived from the connective tissue, bones, and hides of mammals), often retains the alpha-gal epitope and is frequently used in products such as gummy candies, marshmallows, and gelatin desserts.
Individuals with blood group B appear partially protected against sensitization. This protection is likely due to structural similarities between the blood group B antigen and alpha-gal, resulting in the reduced immunologic recognition in B or AB individuals.
Cofactors such as exercise, alcohol, and nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (i.e., Advil, Motrin) and naproxen (i.e., Aleve, Naprosyn) are frequently reported to enhance the likelihood, timing, and/or severity of the reactions. These cofactors may amplify allergic responses by increasing the gastrointestinal absorption of alpha-gal and/or lowering the reaction threshold.
Alpha-gal syndrome differs from the common IgE antibody-mediated food (e.g., nuts, peanuts, fish, shellfish) allergy in 2 important aspects. In a typical food allergy scenario, the individual is sensitized to a particular protein, whereas in alpha-gal syndrome, the individual reacts to a carbohydrate in meats and/or mammalian products. Usually, common food-triggered allergic reactions may cause symptoms within an hour after ingestion, however, clinical manifestations from alpha-gal syndrome are typically delayed, characteristically beginning 2 to 8 hours after exposure to the mammalian product.
The classical manifestations of alpha-gal syndrome may include generalized itching (i.e., pruritus), hives (i.e., urticaria), and/or soft tissue swelling (i.e., angioedema) of the lips, tongue, eyelids, etc. In more severe cases, difficulty in swallowing, shortness of breath, wheezing, and/or life-threatening anaphylaxis may ensue. Gastrointestinal symptoms such as abdominal pain, cramping, nausea, vomiting, and/or diarrhea are also common. The gastrointestinal symptoms are more common in children and may be the sole presenting symptom(s).
The diagnosis rests on a comprehensive history, focusing on symptom timing, dietary exposures, and any history of tick bites. The most commonly used diagnostic test is the measurement of the specific IgE antibody to alpha-gal in a blood sample. A level above 0.1 IU/mL is considered positive and diagnostic. The IgE antibody to alpha-gal testing is the preferred method since skin food prick testing to mammalian meats can be negative in those found to have a positive IgE against alpha-gal. It should be noted that most people with a detectable IgE to alpha-gal will also have detectable IgE to extracts from mammalian meats such as beef, pork, lamb, venison, etc.
If the clinical suspicion for mammalian meat allergy remains high but the initial serum IgE to alpha-gal is negative, then skin prick and serum IgE testing to beef, pork, and lamb may be considered, as this may be helpful with diagnosing other non-alpha-gal forms of meat allergy. As an aside, if the patient primarily reacts to pork, checking for sensitivity to cat via skin prick or serum IgE testing may be warranted to rule out pork-cat syndrome, which is due to cross-reactivity between cat and pork serum albumin.
In order to prevent the development of acute reactions, the core management principle of alpha-gal syndrome is to avoid mammalian meat and associated visceral organs. The mammalian meats usually implicated are beef, pork, lamb and venison, though all non-primate mammalian meat can be causative. Ingestion of meat or products from bison, buffalo, whale, rabbit, horse, goat, and other mammals should also be avoided. Additionally, it is important to highlight to patients that mammalian fats used in cooking (i.e., lard, tallow, casings derived from pork which can be used in poultry-based sausages) are also to be avoided.
Many patients with alpha-gal syndrome will be able to tolerate dairy products. However, if the reactions continue while avoiding meats, dairy products and gelatin-containing foods/medications should also be avoided.
The treatment of reactions depends on the clinical manifestations. Antihistamines may be helpful in treating itching and rashes, but more severe systemic reactions such as anaphylaxis need to be treated with an epinephrine auto-injector (e.g., EpiPen, Auvi-Q, Adrenaclick) or an epinephrine-containing nasal spray such as Neffy. Some reactions may also require intravenous hydration, albuterol inhalation, and/or oxygen supplementation. It should be noted that if an individual uses their epinephrine auto-injector device or their epinephrine-containing nasal spray, they should go immediately to the closest emergency room.
As tick bites have been associated with the development of alpha-gal syndrome, a reasonable prevention tactic is obviously to circumvent sensitization through the avoidance of tick bites. There is data showing that the higher the number of tick bites, the higher the alpha-gal IgE levels, highlighting the importance of avoiding subsequent tick bites after sensitization. Avoiding wooded areas, treating gear with the insecticide permethrin, and using insect repellants will reduce the likelihood of a tick bite. Full body checks should be performed after outdoor activities, and if ticks are found, they should be removed with a fine tipped tweezer.
Some patients with alpha-gal syndrome will be able to tolerate meat again with continued avoidance of recurrent tick bites. In order to determine when and if that person can again tolerate meat, serial monitoring of alpha-gal IgE levels and oral meat challenges may be performed in order to assess the readiness of that individual to consume meat.
The board certified allergists at Black & Kletz Allergy have been diagnosing alpha-gal syndrome for many years. At Black & Kletz Allergy, we treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. Our McLean office location offers a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you think that you have an allergy or sensitivity to meat, we are here to help diagnose your problem and help differentiate whether your symptoms are a meat allergy, meat sensitivity, or alpha-gal syndrome. Black & Kletz Allergy is dedicated to providing the highest quality allergy care in a relaxed, compassionate, and professional environment.
Alpha-gal syndrome is an allergic condition caused by a sensitivity to a carbohydrate known as galactose-alpha-1,3-galactose (i.e., alpha-gal). This molecule is found on the cells of non-primate mammals (i.e., beef, pork, lamb, venison, etc.). This condition is mainly thought to develop after tick bites. The regional distribution of alpha-gal syndrome corresponds with specific tick species populations (e.g., the lone star tick). Alpha-gal syndrome is also called mammalian meat allergy.
In the United States, the prevalence of lone start ticks and alpha-gal syndrome is highest in the Southeast region. Overall, the prevalence of alpha-gal syndrome is thought to be rising, with current estimates suggesting that up to 450,000 cases have occurred in the U.S. since 2010. It was first diagnosed in Virginia.
Other organisms besides ticks have been implicated in the potential induction of alpha-gal sensitization and clinical reactivity. One study demonstrated a correlation between alpha-gal-specific IgE antibody levels and exposure to an intestinal parasite called Ascaris lumbricoides (i.e., round worm). Moreover, some data suggest that bee and wasp stings may also contribute to the production of alpha-gal-specific IgE, particularly in beekeeping populations.
Besides muscle and organ meats, dairy products have also been implicated in triggering reactions. Additionally, gelatin, (commonly derived from the connective tissue, bones, and hides of mammals), often retains the alpha-gal epitope and is frequently used in products such as gummy candies, marshmallows, and gelatin desserts.
Individuals with blood group B appear partially protected against sensitization. This protection is likely due to structural similarities between the blood group B antigen and alpha-gal, resulting in the reduced immunologic recognition in B or AB individuals.
Cofactors such as exercise, alcohol, and nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (i.e., Advil, Motrin) and naproxen (i.e., Aleve, Naprosyn) are frequently reported to enhance the likelihood, timing, and/or severity of the reactions. These cofactors may amplify allergic responses by increasing the gastrointestinal absorption of alpha-gal and/or lowering the reaction threshold.
Alpha-gal syndrome differs from the common IgE antibody-mediated food (e.g., nuts, peanuts, fish, shellfish) allergy in 2 important aspects. In a typical food allergy scenario, the individual is sensitized to a particular protein, whereas in alpha-gal syndrome, the individual reacts to a carbohydrate in meats and/or mammalian products. Usually, common food-triggered allergic reactions may cause symptoms within an hour after ingestion, however, clinical manifestations from alpha-gal syndrome are typically delayed, characteristically beginning 2 to 8 hours after exposure to the mammalian product.
The classical manifestations of alpha-gal syndrome may include generalized itching (i.e., pruritus), hives (i.e., urticaria), and/or soft tissue swelling (i.e., angioedema) of the lips, tongue, eyelids, etc. In more severe cases, difficulty in swallowing, shortness of breath, wheezing, and/or life-threatening anaphylaxis may ensue. Gastrointestinal symptoms such as abdominal pain, cramping, nausea, vomiting, and/or diarrhea are also common. The gastrointestinal symptoms are more common in children and may be the sole presenting symptom(s).
The diagnosis rests on a comprehensive history, focusing on symptom timing, dietary exposures, and any history of tick bites. The most commonly used diagnostic test is the measurement of the specific IgE antibody to alpha-gal in a blood sample. A level above 0.1 IU/mL is considered positive and diagnostic. The IgE antibody to alpha-gal testing is the preferred method since skin food prick testing to mammalian meats can be negative in those found to have a positive IgE against alpha-gal. It should be noted that most people with a detectable IgE to alpha-gal will also have detectable IgE to extracts from mammalian meats such as beef, pork, lamb, venison, etc.
If the clinical suspicion for mammalian meat allergy remains high but the initial serum IgE to alpha-gal is negative, then skin prick and serum IgE testing to beef, pork, and lamb may be considered, as this may be helpful with diagnosing other non-alpha-gal forms of meat allergy. As an aside, if the patient primarily reacts to pork, checking for sensitivity to cat via skin prick or serum IgE testing may be warranted to rule out pork-cat syndrome, which is due to cross-reactivity between cat and pork serum albumin.
In order to prevent the development of acute reactions, the core management principle of alpha-gal syndrome is to avoid mammalian meat and associated visceral organs. The mammalian meats usually implicated are beef, pork, lamb and venison, though all non-primate mammalian meat can be causative. Ingestion of meat or products from bison, buffalo, whale, rabbit, horse, goat, and other mammals should also be avoided. Additionally, it is important to highlight to patients that mammalian fats used in cooking (i.e., lard, tallow, casings derived from pork which can be used in poultry-based sausages) are also to be avoided.
Many patients with alpha-gal syndrome will be able to tolerate dairy products. However, if the reactions continue while avoiding meats, dairy products and gelatin-containing foods/medications should also be avoided.
The treatment of reactions depends on the clinical manifestations. Antihistamines may be helpful in treating itching and rashes, but more severe systemic reactions such as anaphylaxis need to be treated with an epinephrine auto-injector (e.g., EpiPen, Auvi-Q, Adrenaclick) or an epinephrine-containing nasal spray such as Neffy. Some reactions may also require intravenous hydration, albuterol inhalation, and/or oxygen supplementation. It should be noted that if an individual uses their epinephrine auto-injector device or their epinephrine-containing nasal spray, they should go immediately to the closest emergency room.
As tick bites have been associated with the development of alpha-gal syndrome, a reasonable prevention tactic is obviously to circumvent sensitization through the avoidance of tick bites. There is data showing that the higher the number of tick bites, the higher the alpha-gal IgE levels, highlighting the importance of avoiding subsequent tick bites after sensitization. Avoiding wooded areas, treating gear with the insecticide permethrin, and using insect repellants will reduce the likelihood of a tick bite. Full body checks should be performed after outdoor activities, and if ticks are found, they should be removed with a fine tipped tweezer.
Some patients with alpha-gal syndrome will be able to tolerate meat again with continued avoidance of recurrent tick bites. In order to determine when and if that person can again tolerate meat, serial monitoring of alpha-gal IgE levels and oral meat challenges may be performed in order to assess the readiness of that individual to consume meat.
The board certified allergists at Black & Kletz Allergy have been diagnosing alpha-gal syndrome for many years. At Black & Kletz Allergy, we treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. Our McLean office location offers a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you think that you have an allergy or sensitivity to meat, we are here to help diagnose your problem and help differentiate whether your symptoms are a meat allergy, meat sensitivity, or alpha-gal syndrome. Black & Kletz Allergy is dedicated to providing the highest quality allergy care in a relaxed, compassionate, and professional environment.
Allergic to Penicillin Update
December 16, 2025 | Black & Kletz Allergy
 Adverse reactions to medications are very common. Among the drugs associated with immediate hypersensitivity reactions (i.e., IgE antibody-mediated allergic reactions), penicillins are the most commonly observed.
Penicillin allergy is reported in approximately 7 to 10% of the community population and it occurs in up to 20% of hospitalized patients. However, more than 90% of these patients do not have true penicillin allergy, which can be ruled out with the help of a standardized testing procedure. These patients are mislabeled as having a penicillin allergy which can be deleterious to them as penicillins will be avoided in the future for often less effective and more costly alternative antibiotics.
There are 3 common causes for this high rate of false positive penicillin allergy reports:
Adverse reactions to medications are very common. Among the drugs associated with immediate hypersensitivity reactions (i.e., IgE antibody-mediated allergic reactions), penicillins are the most commonly observed.
Penicillin allergy is reported in approximately 7 to 10% of the community population and it occurs in up to 20% of hospitalized patients. However, more than 90% of these patients do not have true penicillin allergy, which can be ruled out with the help of a standardized testing procedure. These patients are mislabeled as having a penicillin allergy which can be deleterious to them as penicillins will be avoided in the future for often less effective and more costly alternative antibiotics.
There are 3 common causes for this high rate of false positive penicillin allergy reports:
- Mislabeling of a side effect (i.e., gastrointestinal upset) as an “allergy”
- Coincidental event (i.e., headache or rash due to an underlying infection)
- Loss of true sensitivity over time with avoidance of penicillins
- Skin prick testing with a small amount of diluted penicillin antigens, that are commercially prepared testing reagents, with negative and positive controls.
- If the prick tests are negative after 20 minutes, a tiny quantity of the antigen is injected into the superficial layers of the skin (i.e., intradermal skin test).
- If the intradermal skin test in the second stage above is also negative after 20 more minutes, the patient will be given 250 mg. of amoxicillin by mouth (i.e., oral challenge) and will be closely monitored for 90 minutes.
Pulmonary Function Testing in VA and DC
December 5, 2025 | Black & Kletz Allergy
 Pulmonary function testing is a tool to help diagnose certain respiratory disorders such as asthma, bronchitis, and emphysema. Bronchitis and emphysema are both categorized as chronic obstructive pulmonary diseases (COPD). A pulmonary function testing doctor McLean, VA knows is Michael R. Kletz, M.D. of Black & Kletz Allergy. He and his colleague, Appaji Gondi, M.D., both perform and interpret pulmonary function tests. The board certified allergists at Black & Kletz Allergy diagnose and treat asthma and other pulmonary (i.e., lung) conditions and have done so for more than 50 years.
A pulmonary function testing doctor McLean, VA trusts is important in the management of asthma. It allows an allergy doctor to not only diagnose asthma, but to follow a patient’s course of asthma. The pulmonary function test helps the allergist choose medications that are needed to control one’s asthma, and it helps the allergy specialist monitor the patient’s progress as well as catch a decline in the patient’s breathing even before it may be noticed by the patient. The earlier that a decline in lung function is discovered, the better the chance to reverse its course quickly so that asthma symptoms do not manifest themselves. In other words, pulmonary function monitoring is a method to prevent asthma symptoms from developing early in its course. It can be utilized to detect subtle changes in lung function before the patient is aware of any increased asthma symptoms. A pulmonary function testing doctor McLean, VA recognizes such as either doctor at Black & Kletz Allergy is thus important for the overall management of asthma and other lung disorders.
Asthma is quite common as approximately 8% of the U.S. population has the diagnosis of asthma. Seeking care with a pulmonary function testing doctor McLean, VA trusts is important in the diagnosis and treatment of asthma. In an undiagnosed individual, a board certified allergist, such as the ones at Black & Kletz Allergy, will begin with a comprehensive history and physical examination. The triggers of one’s asthma will be discussed and if any of the triggers appear to be allergic factors, allergy testing will probably be performed in order to help identify if the person has allergies to those exacerbating factors. Allergy testing may take the form of skin testing or blood testing depending on the history and the circumstances. In addition to allergy testing, a pulmonary function testing doctor McLean, VA residents know will usually order a pulmonary function test to assess lung function, again depending on the situation.
A pulmonary function testing doctor McLean, VA trusts such as the doctors at Black & Kletz Allergy can detect early changes in lung function, such as narrowing of the small airways, that might show a need for a certain medication or a change in a medication as mentioned earlier. Pulmonary function tests may be used to compare one’s lung function with what is expected in individuals without lung disease. They may be utilized to show whether exposure to offending substances in one’s workplace or home environments may have damaged their lungs. Lung function tests are used in order to determine an individual’s ability to tolerate surgery and medical procedures. Pulmonary function tests are primarily used to assess the more common lung disorders such as asthma, chronic bronchitis, chronic obstructive pulmonary diseases (COPD) or emphysema, cystic fibrosis, restrictive lung diseases [e.g., idiopathic pulmonary fibrosis, sarcoidosis, scleroderma (i.e., systemic sclerosis), scoliosis, obesity, myasthenia gravis, hypersensitivity pneumonitis, pneumoconiosis, and restrictive lung disease due to radiation therapy or certain medications (e.g., phenytoin, nitrofurantoin, methotrexate, thiazides, amiodarone, gold, bleomycin, hydralazine, cyclophosphamide)]. Pulmonary function tests are also used to evaluate some conditions that do not stem from the lungs, such as vocal cord dysfunction.
The treatment of asthma may include treating the underlying allergy with allergy medications as well as treating the bronchial tubes and lungs with asthma inhalers. The asthma inhalers may contain a short-acting beta-2 agonist which is a quick-acting bronchodilator, which causes the muscles of the bronchial tubes to relax. These types of inhalers are typically used to mitigate symptoms such as wheezing, coughing, chest tightness, and/or shortness of breath. Inhaled corticosteroids, on the other hand, are usually used to control asthma by reducing inflammation. Inhaled corticosteroids are typically used daily but in certain individuals may also be used on an as needed basis, if prescribed that way by a physician. Combination inhalers (i.e., usually a combination of a corticosteroid plus a long-acting beta-2 agonist) are used for more moderate or severe asthma for longer-term control and relief. In more severe asthmatics, biological medications [e.g. Xolair (i.e., omalizumab), Fasenra (i.e., benralizumab), Nucala (i.e., mepolizumab)] may be utilized. In conglomeration or instead of inhalers depending on the severity of asthma, Singulair (i.e., montelukast), a leukotriene antagonist, is quite effective in the treatment of asthma. In addition to medications, allergy immunotherapy (i.e., allergy shots, allergy injections, allergy hyposensitization) has been very efficacious in the treatment of asthma in allergic individuals. Allergy immunotherapy is effective in about 80-85% of patients who take them. The average length of time on allergy shots is typically 3-5 years.
The board certified allergy specialists at Black & Kletz Allergy treat both pediatric and adult patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. All 3 of our offices have on-site parking. Alternatively, please click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been providing allergy and asthma treatment in the Washington, DC metro area for over 50 years. If you need a pulmonary function testing doctor McLean, VA trusts, please do not hesitate to schedule an appointment.
Pulmonary function testing is a tool to help diagnose certain respiratory disorders such as asthma, bronchitis, and emphysema. Bronchitis and emphysema are both categorized as chronic obstructive pulmonary diseases (COPD). A pulmonary function testing doctor McLean, VA knows is Michael R. Kletz, M.D. of Black & Kletz Allergy. He and his colleague, Appaji Gondi, M.D., both perform and interpret pulmonary function tests. The board certified allergists at Black & Kletz Allergy diagnose and treat asthma and other pulmonary (i.e., lung) conditions and have done so for more than 50 years.
A pulmonary function testing doctor McLean, VA trusts is important in the management of asthma. It allows an allergy doctor to not only diagnose asthma, but to follow a patient’s course of asthma. The pulmonary function test helps the allergist choose medications that are needed to control one’s asthma, and it helps the allergy specialist monitor the patient’s progress as well as catch a decline in the patient’s breathing even before it may be noticed by the patient. The earlier that a decline in lung function is discovered, the better the chance to reverse its course quickly so that asthma symptoms do not manifest themselves. In other words, pulmonary function monitoring is a method to prevent asthma symptoms from developing early in its course. It can be utilized to detect subtle changes in lung function before the patient is aware of any increased asthma symptoms. A pulmonary function testing doctor McLean, VA recognizes such as either doctor at Black & Kletz Allergy is thus important for the overall management of asthma and other lung disorders.
Asthma is quite common as approximately 8% of the U.S. population has the diagnosis of asthma. Seeking care with a pulmonary function testing doctor McLean, VA trusts is important in the diagnosis and treatment of asthma. In an undiagnosed individual, a board certified allergist, such as the ones at Black & Kletz Allergy, will begin with a comprehensive history and physical examination. The triggers of one’s asthma will be discussed and if any of the triggers appear to be allergic factors, allergy testing will probably be performed in order to help identify if the person has allergies to those exacerbating factors. Allergy testing may take the form of skin testing or blood testing depending on the history and the circumstances. In addition to allergy testing, a pulmonary function testing doctor McLean, VA residents know will usually order a pulmonary function test to assess lung function, again depending on the situation.
A pulmonary function testing doctor McLean, VA trusts such as the doctors at Black & Kletz Allergy can detect early changes in lung function, such as narrowing of the small airways, that might show a need for a certain medication or a change in a medication as mentioned earlier. Pulmonary function tests may be used to compare one’s lung function with what is expected in individuals without lung disease. They may be utilized to show whether exposure to offending substances in one’s workplace or home environments may have damaged their lungs. Lung function tests are used in order to determine an individual’s ability to tolerate surgery and medical procedures. Pulmonary function tests are primarily used to assess the more common lung disorders such as asthma, chronic bronchitis, chronic obstructive pulmonary diseases (COPD) or emphysema, cystic fibrosis, restrictive lung diseases [e.g., idiopathic pulmonary fibrosis, sarcoidosis, scleroderma (i.e., systemic sclerosis), scoliosis, obesity, myasthenia gravis, hypersensitivity pneumonitis, pneumoconiosis, and restrictive lung disease due to radiation therapy or certain medications (e.g., phenytoin, nitrofurantoin, methotrexate, thiazides, amiodarone, gold, bleomycin, hydralazine, cyclophosphamide)]. Pulmonary function tests are also used to evaluate some conditions that do not stem from the lungs, such as vocal cord dysfunction.
The treatment of asthma may include treating the underlying allergy with allergy medications as well as treating the bronchial tubes and lungs with asthma inhalers. The asthma inhalers may contain a short-acting beta-2 agonist which is a quick-acting bronchodilator, which causes the muscles of the bronchial tubes to relax. These types of inhalers are typically used to mitigate symptoms such as wheezing, coughing, chest tightness, and/or shortness of breath. Inhaled corticosteroids, on the other hand, are usually used to control asthma by reducing inflammation. Inhaled corticosteroids are typically used daily but in certain individuals may also be used on an as needed basis, if prescribed that way by a physician. Combination inhalers (i.e., usually a combination of a corticosteroid plus a long-acting beta-2 agonist) are used for more moderate or severe asthma for longer-term control and relief. In more severe asthmatics, biological medications [e.g. Xolair (i.e., omalizumab), Fasenra (i.e., benralizumab), Nucala (i.e., mepolizumab)] may be utilized. In conglomeration or instead of inhalers depending on the severity of asthma, Singulair (i.e., montelukast), a leukotriene antagonist, is quite effective in the treatment of asthma. In addition to medications, allergy immunotherapy (i.e., allergy shots, allergy injections, allergy hyposensitization) has been very efficacious in the treatment of asthma in allergic individuals. Allergy immunotherapy is effective in about 80-85% of patients who take them. The average length of time on allergy shots is typically 3-5 years.
The board certified allergy specialists at Black & Kletz Allergy treat both pediatric and adult patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. All 3 of our offices have on-site parking. Alternatively, please click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been providing allergy and asthma treatment in the Washington, DC metro area for over 50 years. If you need a pulmonary function testing doctor McLean, VA trusts, please do not hesitate to schedule an appointment.
Type 2 Inflammation
November 27, 2025 | Black & Kletz Allergy
 The human immune system has evolved to defend and protect us from infections caused by microbes and some types of cancers. The cells responsible for these defenses originate in the bone marrow and circulate in the blood stream and lymphatic system.
The human immune system has evolved to defend and protect us from infections caused by microbes and some types of cancers. The cells responsible for these defenses originate in the bone marrow and circulate in the blood stream and lymphatic system.
Classically, host immunity is divided into innate and adaptive immune responses. The former reacts rapidly and non-specifically to pathogens, whereas the latter responds in a slower but specific manner, with the generation of long-lived immunological memory.
Innate immunity is mediated by immune cell populations such as myeloid cells, natural killer (NK) cells, innate lymphoid cells, and complement. Adaptive immunity is a relatively new evolutionary trait based on the immunoglobulin family (i.e., antibodies) and cells such as B- and T-lymphocytes.
During an infection, the innate immunity is the first to be triggered (i.e., the inflammatory reaction), taking no longer than minutes to hours to be fully activated. This is crucial for the host defense in the first phase of a new infection. While innate immunity is generally able to eliminate the pathogens efficiently, initial clearance of an infection can fail due to the high number or virulence of the invading pathogens. In these situations, lymphocytes and adaptive immune mechanisms are activated, which allows for specific recognition and elimination of the pathogen. The establishment of the adaptive immunity requires approximately 1–2 weeks and is important for host defense during the latter phases of an infection as well as secondary infections due to its capacity to “remember” and respond more effectively to restimulation.
Adaptive immunity is further subdivided into 2 types: humoral and cellular. Humoral immunity is mediated by antibodies which are also known as immunoglobulins. These antibodies are secreted by B-cells or B-lymphocytes. They are called B-lymphocytes because they are made in the bone marrow. Cellular immunity is mediated by in the thymus and thus named T-cells or T-lymphocytes.
T-lymphocytes have 2 main sub-populations called T-helper 1 cells (Th-1) and T-helper 2 cells (Th-2 cells). The main role of Th-1 cells is to defend against intracellular pathogens whereas Th-2 cells are mainly involved in defenses against large extracellular organisms such as parasites. These 2 cells fight infections and infestations by secreting different types of effector molecules called cytokines.
As we are now living in a more hygienic environment than our ancestors, we are encountering fewer water-borne pathogens such as parasites. As a result, the Th-2 cells, due to mysterious reasons, instead of fighting the parasites and pathogens, are now reacting against harmless substances such as pollen, dust mites, mold spores, food proteins, etc., mistaking them as potentially harmful.
Over the years, this evolutionary happening has now resulted in allergic diseases being mediated by “Type 2 inflammation.” This phenomenon is responsible for the “atopic march” which begins in infancy as eczema (i.e., atopic dermatitis) and evolving to affect various organs in later life.
Atopic dermatitis manifests in the skin and is characterized by itching, dryness, and inflammation of the skin. It is usually genetically determined by mutations in genes such as “filagrin.” The chronic inflammation of the skin leads to defects in the barrier functions of the skin, allowing easier access for foreign proteins into the body.
The other manifestations of Type 2 inflammation depend on the organ systems involved. Allergic rhinitis impacts the nasal passages and leads to
symptoms such as sneezing, nasal congestion, runny nose, post-nasal drip, watery eyes, red eyes, and/or itchy eyes. Asthma primarily impacts the lungs and causes airway inflammation, hyperreactivity, and wheezing.
Chronic rhinosinusitis with nasal polyps affects the upper airways leading to nasal obstruction, loss of smell, and persistent sinus infections. Eosinophilic esophagitis (EoE) impacts the gastrointestinal tract and can lead to difficulty swallowing, food impaction, and inflammation of the esophagus, whereas food allergies are a more systemic manifestation that may involve multiple organ systems and lead to reactions ranging from mild hives to life-threatening anaphylaxis.
All of the above conditions have the common thread of Type 2 inflammation. They present differently, though, depending on which tissues are primarily affected, it is important to recognize early signs. It is important for allergists to know the connections because we can then diagnose them earlier. This allows the allergy specialists to better anticipate the course of various allergic and immunologic diseases and possibly even interrupt the atopic march leading to a decrease in allergic symptoms in the patient.
The board certified allergists at Black & Kletz Allergy have 3 office locations in the Washington, Northern Virginia, and Maryland metropolitan area. The allergy doctors at Black & Kletz Allergy treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking and both the Washington, DC and McLean, VA offices are Metro accessible. In addition, the McLean, VA office has a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. The allergy specialists at Black & Kletz Allergy have been helping patients with hay fever, food allergies, asthma, eczema, hives, sinus disease, insect sting allergies, immunological disorders, and medication allergies for over 50 years. We understand the underlying type 2 inflammation that comes along with allergies and asthma and we aim to decrease or eliminate it. If you suffer from any allergy or immune problem, it is our mission to improve your quality of life by reducing or preventing your unwanted and annoying allergy symptoms.
The human immune system has evolved to defend and protect us from infections caused by microbes and some types of cancers. The cells responsible for these defenses originate in the bone marrow and circulate in the blood stream and lymphatic system.
The human immune system has evolved to defend and protect us from infections caused by microbes and some types of cancers. The cells responsible for these defenses originate in the bone marrow and circulate in the blood stream and lymphatic system.
Classically, host immunity is divided into innate and adaptive immune responses. The former reacts rapidly and non-specifically to pathogens, whereas the latter responds in a slower but specific manner, with the generation of long-lived immunological memory.
Innate immunity is mediated by immune cell populations such as myeloid cells, natural killer (NK) cells, innate lymphoid cells, and complement. Adaptive immunity is a relatively new evolutionary trait based on the immunoglobulin family (i.e., antibodies) and cells such as B- and T-lymphocytes.
During an infection, the innate immunity is the first to be triggered (i.e., the inflammatory reaction), taking no longer than minutes to hours to be fully activated. This is crucial for the host defense in the first phase of a new infection. While innate immunity is generally able to eliminate the pathogens efficiently, initial clearance of an infection can fail due to the high number or virulence of the invading pathogens. In these situations, lymphocytes and adaptive immune mechanisms are activated, which allows for specific recognition and elimination of the pathogen. The establishment of the adaptive immunity requires approximately 1–2 weeks and is important for host defense during the latter phases of an infection as well as secondary infections due to its capacity to “remember” and respond more effectively to restimulation.
Adaptive immunity is further subdivided into 2 types: humoral and cellular. Humoral immunity is mediated by antibodies which are also known as immunoglobulins. These antibodies are secreted by B-cells or B-lymphocytes. They are called B-lymphocytes because they are made in the bone marrow. Cellular immunity is mediated by in the thymus and thus named T-cells or T-lymphocytes.
T-lymphocytes have 2 main sub-populations called T-helper 1 cells (Th-1) and T-helper 2 cells (Th-2 cells). The main role of Th-1 cells is to defend against intracellular pathogens whereas Th-2 cells are mainly involved in defenses against large extracellular organisms such as parasites. These 2 cells fight infections and infestations by secreting different types of effector molecules called cytokines.
As we are now living in a more hygienic environment than our ancestors, we are encountering fewer water-borne pathogens such as parasites. As a result, the Th-2 cells, due to mysterious reasons, instead of fighting the parasites and pathogens, are now reacting against harmless substances such as pollen, dust mites, mold spores, food proteins, etc., mistaking them as potentially harmful.
Over the years, this evolutionary happening has now resulted in allergic diseases being mediated by “Type 2 inflammation.” This phenomenon is responsible for the “atopic march” which begins in infancy as eczema (i.e., atopic dermatitis) and evolving to affect various organs in later life.
Atopic dermatitis manifests in the skin and is characterized by itching, dryness, and inflammation of the skin. It is usually genetically determined by mutations in genes such as “filagrin.” The chronic inflammation of the skin leads to defects in the barrier functions of the skin, allowing easier access for foreign proteins into the body.
The other manifestations of Type 2 inflammation depend on the organ systems involved. Allergic rhinitis impacts the nasal passages and leads to
symptoms such as sneezing, nasal congestion, runny nose, post-nasal drip, watery eyes, red eyes, and/or itchy eyes. Asthma primarily impacts the lungs and causes airway inflammation, hyperreactivity, and wheezing.
Chronic rhinosinusitis with nasal polyps affects the upper airways leading to nasal obstruction, loss of smell, and persistent sinus infections. Eosinophilic esophagitis (EoE) impacts the gastrointestinal tract and can lead to difficulty swallowing, food impaction, and inflammation of the esophagus, whereas food allergies are a more systemic manifestation that may involve multiple organ systems and lead to reactions ranging from mild hives to life-threatening anaphylaxis.
All of the above conditions have the common thread of Type 2 inflammation. They present differently, though, depending on which tissues are primarily affected, it is important to recognize early signs. It is important for allergists to know the connections because we can then diagnose them earlier. This allows the allergy specialists to better anticipate the course of various allergic and immunologic diseases and possibly even interrupt the atopic march leading to a decrease in allergic symptoms in the patient.
The board certified allergists at Black & Kletz Allergy have 3 office locations in the Washington, Northern Virginia, and Maryland metropolitan area. The allergy doctors at Black & Kletz Allergy treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking and both the Washington, DC and McLean, VA offices are Metro accessible. In addition, the McLean, VA office has a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. The allergy specialists at Black & Kletz Allergy have been helping patients with hay fever, food allergies, asthma, eczema, hives, sinus disease, insect sting allergies, immunological disorders, and medication allergies for over 50 years. We understand the underlying type 2 inflammation that comes along with allergies and asthma and we aim to decrease or eliminate it. If you suffer from any allergy or immune problem, it is our mission to improve your quality of life by reducing or preventing your unwanted and annoying allergy symptoms.
Food Allergies and Thanksgiving
November 12, 2025 | Black & Kletz Allergy
 Well, it is that time of year again. A time for getting together with family and friends for the annual ritual of gluttony - I mean Thanksgiving. Although the holiday is generally a festive occasion, some food-allergic individuals find Thanksgiving to be a time of the year where they are more concerned than usual. Individuals with food allergies are always concerned when eating at a restaurant or at someone’s house due to the fear of consuming food that causes them to have food allergy symptoms. On Thanksgiving, however, this fear is intensified because typically the food offered on Thanksgiving at someone’s home is usually made by many different people. Normally, when it is not Thanksgiving, the allergic individual can tell the host/hostess what food allergies they have, and the host/hostess will avoid serving that food or foods. On Thanksgiving however, since there are usually multiple people either preparing or cooking the meal, there is more of a chance that an allergic ingredient will be used simply because the person making the food either was not told about the food allergy, they forgot to avoid using it, or it was not communicated to them about the food allergy by the host/hostess. As a result, more mistakes may be made, and a person is more likely to eat food that he or she is allergic to than in other more intimate gatherings.
Common food allergens such as milk, egg, wheat, soy, peanuts, and tree nuts are often found around the Thanksgiving table. Gravy, used for turkey and mashed potatoes, frequently contains the food allergens dairy, soy, and/or wheat. Tree nuts (e.g., almonds) are frequently found on string beans and in some types of stuffing (e.g., chestnuts). Tree nuts and peanuts are common in many desserts such as brownies and pecan pie. Milk (i.e., dairy) and eggs are also used in many baked goods. Although pumpkin allergies are not common, pumpkin pie may contain a host of ingredients that may induce a food allergy in some sensitive individuals. It is significant to note that among various cultures, many families incorporate many ethnic foods in their celebrations. These foods may not be traditional, but they may increase the probability of other allergenic foods such as shellfish, fish, etc. to be the cause of an imminent food allergy. If a person has a serious food allergy, it is sensible for that individual to bring their own food, so they can avoid any potential allergic reaction from food.
Although having an allergy to turkey does exit, it is not a common food allergy. It is worth noting however that many people feel sleepy after consuming turkey, particularly on Thanksgiving when large amounts are typically eaten. The reason for the sleepiness may stem from the fact that turkey contains higher levels of the amino acid “L-tryptophan.” The amino acid L-tryptophan is an essential amino acid that has to be obtained from foods we eat since the body does not make L-tryptophan on its own. Amino acids are the precursors to proteins and it takes many amino acids to create a protein. Thus, amino acids are considered to be the “building blocks” of proteins. It is also important to mention that there are many other foods besides turkey that are rich in L-tryptophan. Some of these foods include oats, eggs, canned tuna, fish, legumes (e.g., soybeans, peanuts, lima beans), milk, cheese, yogurt, seeds (e.g., pumpkin, sunflower, sesame), bread, chocolate, and some fruits. It should be stated that turkey and chicken both have comparable amounts of L-tryptophan. Another thought-provoking fact is that the dark turkey meat has less of the amino acid L-tryptophan than the white turkey meat, but with chicken, it is the opposite, as there is less L-tryptophan in white chicken meat than dark chicken meat. After eating turkey, the L-tryptophan will enter one’s bloodstream from the digestive tract and travel to the brain where it gets converted to the chemical “serotonin.” It is the serotonin that is responsible for causing the sleepiness associated with eating turkey. It should also be pointed out that eating a high carbohydrate, high fat meal can also lead to sleepiness and fatigue about 1-2 hours after eating. Serotonin, however, is a chemical in the brain that plays a role in one’s mood, as well as pain intolerance. High serotonin levels are associated with elevated moods and a sense of relaxation. Serotonin may also increase one’s pain tolerance. In addition, L-tryptophan is thought to have a beneficial effect on learning, memory, and depression. Serotonin may also have useful effects on decreasing anxiety, premenstrual pain, and seasonal affective disorder although more research is needed to verify this. So, if you experience sleepiness at the Thanksgiving Day table, it may not be your in-laws at all, it may be the turkey! Likewise, if you are in a good mood and feel less depressed during Thanksgiving, it may be that you are happy to be with family, but it still could be the turkey!
The board certified allergists at Black & Kletz Allergy diagnose and treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. You may also click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been a fixture in the greater Washington, DC, Northern Virginia, and Maryland metropolitan community for over 50 years for our outstanding services for the diagnosis and treatment of allergic, asthmatic, and immunological conditions.
Well, it is that time of year again. A time for getting together with family and friends for the annual ritual of gluttony - I mean Thanksgiving. Although the holiday is generally a festive occasion, some food-allergic individuals find Thanksgiving to be a time of the year where they are more concerned than usual. Individuals with food allergies are always concerned when eating at a restaurant or at someone’s house due to the fear of consuming food that causes them to have food allergy symptoms. On Thanksgiving, however, this fear is intensified because typically the food offered on Thanksgiving at someone’s home is usually made by many different people. Normally, when it is not Thanksgiving, the allergic individual can tell the host/hostess what food allergies they have, and the host/hostess will avoid serving that food or foods. On Thanksgiving however, since there are usually multiple people either preparing or cooking the meal, there is more of a chance that an allergic ingredient will be used simply because the person making the food either was not told about the food allergy, they forgot to avoid using it, or it was not communicated to them about the food allergy by the host/hostess. As a result, more mistakes may be made, and a person is more likely to eat food that he or she is allergic to than in other more intimate gatherings.
Common food allergens such as milk, egg, wheat, soy, peanuts, and tree nuts are often found around the Thanksgiving table. Gravy, used for turkey and mashed potatoes, frequently contains the food allergens dairy, soy, and/or wheat. Tree nuts (e.g., almonds) are frequently found on string beans and in some types of stuffing (e.g., chestnuts). Tree nuts and peanuts are common in many desserts such as brownies and pecan pie. Milk (i.e., dairy) and eggs are also used in many baked goods. Although pumpkin allergies are not common, pumpkin pie may contain a host of ingredients that may induce a food allergy in some sensitive individuals. It is significant to note that among various cultures, many families incorporate many ethnic foods in their celebrations. These foods may not be traditional, but they may increase the probability of other allergenic foods such as shellfish, fish, etc. to be the cause of an imminent food allergy. If a person has a serious food allergy, it is sensible for that individual to bring their own food, so they can avoid any potential allergic reaction from food.
Although having an allergy to turkey does exit, it is not a common food allergy. It is worth noting however that many people feel sleepy after consuming turkey, particularly on Thanksgiving when large amounts are typically eaten. The reason for the sleepiness may stem from the fact that turkey contains higher levels of the amino acid “L-tryptophan.” The amino acid L-tryptophan is an essential amino acid that has to be obtained from foods we eat since the body does not make L-tryptophan on its own. Amino acids are the precursors to proteins and it takes many amino acids to create a protein. Thus, amino acids are considered to be the “building blocks” of proteins. It is also important to mention that there are many other foods besides turkey that are rich in L-tryptophan. Some of these foods include oats, eggs, canned tuna, fish, legumes (e.g., soybeans, peanuts, lima beans), milk, cheese, yogurt, seeds (e.g., pumpkin, sunflower, sesame), bread, chocolate, and some fruits. It should be stated that turkey and chicken both have comparable amounts of L-tryptophan. Another thought-provoking fact is that the dark turkey meat has less of the amino acid L-tryptophan than the white turkey meat, but with chicken, it is the opposite, as there is less L-tryptophan in white chicken meat than dark chicken meat. After eating turkey, the L-tryptophan will enter one’s bloodstream from the digestive tract and travel to the brain where it gets converted to the chemical “serotonin.” It is the serotonin that is responsible for causing the sleepiness associated with eating turkey. It should also be pointed out that eating a high carbohydrate, high fat meal can also lead to sleepiness and fatigue about 1-2 hours after eating. Serotonin, however, is a chemical in the brain that plays a role in one’s mood, as well as pain intolerance. High serotonin levels are associated with elevated moods and a sense of relaxation. Serotonin may also increase one’s pain tolerance. In addition, L-tryptophan is thought to have a beneficial effect on learning, memory, and depression. Serotonin may also have useful effects on decreasing anxiety, premenstrual pain, and seasonal affective disorder although more research is needed to verify this. So, if you experience sleepiness at the Thanksgiving Day table, it may not be your in-laws at all, it may be the turkey! Likewise, if you are in a good mood and feel less depressed during Thanksgiving, it may be that you are happy to be with family, but it still could be the turkey!
The board certified allergists at Black & Kletz Allergy diagnose and treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. You may also click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been a fixture in the greater Washington, DC, Northern Virginia, and Maryland metropolitan community for over 50 years for our outstanding services for the diagnosis and treatment of allergic, asthmatic, and immunological conditions.
Our Doctors have been featured in both the National and Local News









