
Mast Cell Conditions
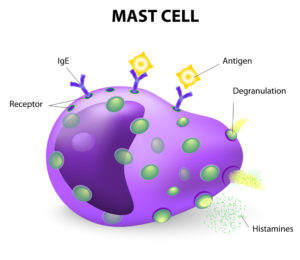
Mast cells are a type of white blood cells. They are an important part of our immune system as they help us fight off infections and other invaders. Mast cells contain granules which contain a variety of chemical substances (e.g., histamine, heparin, tryptase, serotonin, leukotrienes, prostaglandins, cytokines). These chemical substances have effects on the body such as inflammation and allergic symptoms.
Mast cells play a crucial role in defending us against infections and aiding in wound healing. Despite these important functions, they can also cause diseases when too many of them are produced (i.e., mastocytosis) or when they become overactive (i.e., mast cell activation syndrome). These fairly uncommon conditions occur in approximately 1 in every 150,000 individuals.
Cause:
The exact cause of these mast cell conditions is unknown. It is however thought that abnormal genes inherited from parents could play a role in the development of mast cell disorders.
Symptoms:
Mast cell disorders can affect various organs in the body:
1. Skin: The skin is the largest organ in our bodies. When excessive numbers of mast cells are deposited in the skin, they cause a condition called urticaria pigmentosa, which manifests as light brown, itchy, and raised patches over various parts of the body. If the patches are rubbed, they become redder, swollen, and may result in blisters (i.e., Darier’s sign). Some individuals also develop dermatographism, which is a condition where one is able to write on the skin with a blunt object. Urticaria pigmentosa is more prevalent in children and usually improves with age. Frequent episodes of flushing, especially over the face, is a common symptom. Generalized itching (i.e., pruritus) can be a very bothersome symptom, interfering with both sleep and work. In addition, the localized accumulation of mast cells can present as nodules.
2. Gastrointestinal: Abdominal pain, bloating, discomfort after eating, heartburn, nausea, vomiting, pale stools
3. Cardiovascular: Decreased blood pressure, lightheadedness, fainting
4. Bone Marrow: Anemia, bone pain, fractures.
5. Respiratory: Wheezing, shortness of breath, coughing
6. Neurologic: Headache, tremors, numbness
7. Lymphatic: Swelling of lymph nodes, liver, spleen and other organs
Triggers:
A number of factors can trigger symptoms of mast cell disorders:
1. Physical: Heat, cold, friction, sunlight, fever, fatigue, physical exertion
2. Emotional stress
3. Food: Cheese, spices, shellfish, food preservatives (e.g., MSG), food additives (e.g., flavorings, colorings)
4. Infections: Bacteria, viruses, fungi
5. Drugs: Aspirin, antibiotics, anesthetics, opioids, alcohol
6. Insect bites or stings
7. Irritants: Strong odors, perfumes, other chemical irritants
8. Surgery
Diagnosis:
1. Blood tests: Measure tryptase levels at the baseline (i.e., before flare-up) and during a flare-up when tryptase levels are more likely to be elevated.
2. Urine tests: Measure the metabolic end products of tryptase
3. Bone marrow biopsy: Microscopic examination of the bone marrow for evidence of mast cell deposition
4. Skin biopsy: Microscopic examination of skin lesions
5. Genetic tests: Looks for gene abnormalities
6. Chest and bone X-rays or scans
7. Skin prick tests: Detects specific IgE antibodies to environmental and/or food allergens, if suggested by history of flare-ups on exposure
Treatment:
Unfortunately, there is no cure for these disorders but various manifestations can be treated in order to help relieve the symptoms as well as help preserve the function of organs systems.
1. Acute severe systemic reactions (i.e., anaphylaxis) are treated with an immediate epinephrine injection. Patients should to carry an epinephrine auto-injector (e.g., EpiPen, Auvi-Q, Adrenaclick) and wear a medical alert bracelet. If used, it is important for the individual to go to the closest emergency room.
2. Itching, flushing, and other skin allergy symptoms can be controlled by using H1-blocking antihistamines such as Claritin (loratadine), Allegra (fexofenadine), and Zyrtec (cetirizine) in combination with H2-blockers such as Tagamet (cimetidine) or Pepcid (famotidine).
3. Medications which stabilize the mast cells such as cromolyn, nedocromil, and ketotifen can help prevent from degranulation of the granules inside mast cells and thus help prevent the release of chemical mediators into the tissues and the bloodstream. These medications are often used to treat gastrointestinal symptoms such as nausea, vomiting, and abdominal cramping.
4. Digestive symptoms caused by mast cell disorders can also be improved with proton pump inhibitor (PPI) medications such as Prilosec (omeprazole), Prevacid (lansoprazole), and Nexium (esomeprazole).
5. Albuterol inhalers will help open the airways and help wheezing, coughing and/or shortness of breath in individuals with respiratory symptoms.
6. Anticholinergic medications may be used to reduce the motility of the bowels which may help control diarrhea.
7. Anti-inflammatory medications such as corticosteroids (e.g., prednisone) and leukotriene antagonists [e.g., Singulair (montelukast), Accolate (zafirlukast), Zyflo (zileuton)] are sometimes used to help control systemic symptoms. Topical corticosteroid creams or ointments, as well as phototherapy can improve localized skin lesions.
8. Surgical removal of the spleen can help improve severe symptoms in some individuals.
9. Immune modulating medications such as interferons may be used in more severe cases of systemic mastocytosis
10. Bone marrow transplant may be necessary in severe cases of systemic mastocytosis.
11. Stem cell therapy may be necessary in severe cases of systemic mastocytosis.
Prognosis:
Most cases of localized mast cell disease can persist for many years as nodules on the skin. In rare instances, cancers can develop which require constant monitoring.
Systemic mastocytosis tends to be persistent at a low level for decades, requiring treatment to control symptoms. Occasionally, however, it can become aggressive and even life-threatening.
Avoidance of exposure to the known triggers, as best as possible, can help minimize the symptoms and reduce the need for medications.
The board certified allergy specialists at Black & Kletz Allergy treat both adult and pediatric patients. We have been diagnosing and treating mast cell diseases for many years. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our offices have on-site parking. In addition, the Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. To schedule an appointment, please click Request an Appointment and we will respond within 24 hours by the next business day. The allergists at Black & Kletz Allergy have been the trusted allergists in the greater Washington, DC and Northern Virginia community for over 50 years. We pride ourselves for our outstanding services we provide for the diagnosis and treatment of mast cell disorders as well as other conditions in the fields of allergy, asthma, and immunology.
 Spring is in the air and many individuals are suffering. Although many are experiencing the signs and symptoms of
Spring is in the air and many individuals are suffering. Although many are experiencing the signs and symptoms of  Dust mites are one of the most common triggers of allergic conditions such as in the conditions of
Dust mites are one of the most common triggers of allergic conditions such as in the conditions of  Later this month, Spring is officially here. Along with the warmer weather and longer days comes the pollination of trees and grasses. For some allergy sufferers, the presence of tree and grass pollens can be a miserable sight as these pollens may cause an array of allergy and asthma symptoms that are very annoying.
Later this month, Spring is officially here. Along with the warmer weather and longer days comes the pollination of trees and grasses. For some allergy sufferers, the presence of tree and grass pollens can be a miserable sight as these pollens may cause an array of allergy and asthma symptoms that are very annoying. Oral allergy syndrome (also known as pollen food allergy syndrome) affects approximately one third of people with seasonal
Oral allergy syndrome (also known as pollen food allergy syndrome) affects approximately one third of people with seasonal  Bug bites are certainly very common. Almost everyone has been bitten by a bug in their lifetime and almost everyone has had at least a minor local reaction to the bug bite. In some instances, an individual may have a more severe reaction that is not an allergic reaction but it can mimic an allergic reaction. In other cases, however, an individual may actually have a true allergic reaction. In order to differentiate between an allergic reaction and a non-allergic reaction, a consultation with a
Bug bites are certainly very common. Almost everyone has been bitten by a bug in their lifetime and almost everyone has had at least a minor local reaction to the bug bite. In some instances, an individual may have a more severe reaction that is not an allergic reaction but it can mimic an allergic reaction. In other cases, however, an individual may actually have a true allergic reaction. In order to differentiate between an allergic reaction and a non-allergic reaction, a consultation with a 
 As we enter into the Winter months, a sensitivity to cold temperatures may trigger some allergic reactions in susceptible individuals. Below are some conditions where exposure to cold can cause clinical disease.
As we enter into the Winter months, a sensitivity to cold temperatures may trigger some allergic reactions in susceptible individuals. Below are some conditions where exposure to cold can cause clinical disease.