Every year, several children are taken to emergency departments on Halloween day for the management of severe allergic reactions. What is meant to be a fun-filled activity can turn out to be a harrowing experience for some families. A few general precautions made by families can prevent most allergic emergencies in children and are as follows:
Many families understand how to read labels on foods and avoid those that contain ingredients that their children are sensitized to. However, most “fun-sized” candies handed out while trick-or-treating either do not have any labeling at all or they may contain different ingredients than regular sized packages.
Preventing children with food allergies to trick-or-treat without adult supervision as well as avoiding candies without proper labeling can prevent a life-threatening reaction. It is a good practice for severely allergic individuals to carry epinephrine self-injectable devices (e.g., EpiPen, Auvi-Q, Adrenaclick) while trick or treating.
Children with food allergies should be taught to politely refuse homemade foods such as cookies and cupcakes that may be unsafe for them.
Ragweed and mold spores are the most common environmental aeroallergens in the Fall in many geographical areas in late October. In addition, exposure to cats and dogs are not uncommon while trick or treating. Exposure to these allergens may trigger allergic rhinitis (i.e., hay fever) and/or severe respiratory allergic reactions. The use of allergy and/or asthma medications before heading out may be protective. Showering, washing one’s hair, and changing into fresh new clothes after trick or treating will reduce airborne allergen exposure.
Cold air is a known irritant and prolonged exposure to cold air may aggravate asthma in susceptible children. Frequent indoor breaks and covering the nose and mouth while outdoors can minimize this risk. Children with a history of asthma should also take their rescue inhalers with them while trick-or-treating.
Haunted houses with smoke machines may pose a danger to children and adults with severe asthma. Exposure to smoke of any kind can cause an acute asthma exacerbation. Preparation and avoidance are necessary in order to prevent severe asthma attacks.
Halloween costumes containing strong chemicals may be irritating to children with sensitive skin and as a result a flare-up of their eczema (i.e., atopic dermatitis) may occur. Latex-containing masks as part of the costume may be especially deleterious to children with a history of latex allergy. Children with a sensitivity to metals such as nickel may be exposed to nickel buttons and buckles in costumes which may lead to itching and skin rashes
To help insure that a food allergic child can participate in Halloween and have as much fun as the next child, although nothing is guaranteed, there is a program run by theFood Allergy Research and Education (FARE) organization called the “Teal Pumpkin Project”. This FARE-sponsored international program has been in place since 2014. It began in Tennessee by the mother of a severely food allergic child. The Teal Pumpkin Project’s purpose is to raise awareness of the severity of food allergies and show support to families who have food allergic children. This is done by painting a pumpkin the color teal and then placing it on one’s front porch to signify that “non-food” treats are available at that location on Halloween night. The color teal is used because it represents food allergy awareness. Typically, “non-food” treats may include toys, crayons, stickers, rings, bracelets, necklaces, glow sticks, hair accessories, coins, finger puppets, balls, bookmarks, spider rings, vampire fangs, whistles, etc.
It important to point out that the Teal Pumpkin Project is not exclusionary and it still promotes the option of distributing normal trick-or-treat candy to children without food allergies. It recommends that the “non-food” items be kept in a different bowl than the traditional candy bowl. FARE provides a “Teal Pumpkin Project Participation Map” on its website so that participating houses can be easily assessed by the parents of food allergic children.
Being cognizant of the hidden dangers of trick-or-treating and proactive in preventing allergen exposures can greatly reduce parents’ anxiety as well as help children fully enjoy the Halloween experience. The board certified allergists at Black & Kletz Allergy have had over 5 decades of experience in diagnosing and managing food and environmental allergies, asthma, and eczema in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Both food and environmental allergies can be diagnosed by a thorough history and physical examination along with prick skin testing and/or blood testing. We would be happy to see you in one of our 3 convenient locations with offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. There is on-site parking at each location and both the Washington, DC and McLean, VA offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call our office or alternatively, you may click Request an Appointment and we will respond within 24 hours on the next business day. Black & Kletz Allergy is proud to provide quality allergy, asthma, and immunology care in a relaxed compassionate environment.
There is some exciting news for children and their families with a history of peanut allergies. On September 13, 2019, the Allergenic Products Advisory Committee of the Food and Drug Administration (FDA) voted to recommend approval of a new oral immunotherapy product for children with peanut allergy.
Peanut is one of the most common foods that can be allergenic in children. It is also responsible for more severe and occasionally life-threatening reactions in highly sensitive children and adults. Adding to the concerns, in the U.S., peanut allergy in children has increased 21% since 2010, and nearly 2.5% of U.S. children may have an allergy to peanuts.
The current standard of care for the treatment of food allergies is the avoidance of the allergen (e.g., peanut) in conjunction with the treatment of anaphylaxis with self-injectable epinephrine devices (e.g., EpiPen, Auvi-Q, and/or Adrenaclick). It should be noted that parents of children with severe sensitivity to peanut live with constant fear of a life-threatening reaction triggered by an accidental exposure to peanut products.
Oral immunotherapy (OIT) refers to feeding an allergic individual an increasing amount of an allergen with the goal of increasing the threshold that triggers a reaction. The procedure entails feeding the allergenic food to the child, beginning with an extremely small dose and gradually increasing the dose at regular intervals while closely monitoring for adverse reactions. This must be done by in a hospital or in an allergist’s office where the allergist and staff are prepared to treat an adverse reaction without delay. The “escalation” of doses, as mentioned above, is typically performed in an allergist’s office, which is equipped to monitor and treat potential reactions whereas maintenance doses can be given at home.
“Desensitization” refers to the improvement in food challenge outcomes after therapy and relies on ongoing exposure to the allergen. If successfully accomplished, desensitization has the potential to substantially reduce the risk of a severe reaction following accidental exposure to the allergen and would hopefully minimize the anxiety of parents. This form of treatment also requires regular exposure to the food indefinitely in order to maintain the “desensitized” or “tolerant” state. OIT with peanut is unlikely to induce “sustained unresponsiveness” which refers to the retention of the protective benefit achieved through therapy. This sustained unresponsiveness is not reliant on the ongoing exposure to peanut.
The possible side effects of OIT include symptoms limited to the gastrointestinal tract such as itching of the mouth and/or lips, abdominal cramping, and diarrhea. Rarely more severe systemic reactions such as generalized hives (i.e., urticaria), swelling of tongue and/or throat (i.e., angioedema), difficulty in swallowing, shortness of breath, wheezing, and drop in blood pressure may occur.
The FDA has not yet approved the new treatment but they are likely to approve it soon based on the recommendations of its Allergenic Products Advisory Committee. “Palforzia” will be the brand name of the new drug, which is a powder containing 12 peanut proteins (Ara h 1, Ara h 2, Ara h 3, etc.) thought to be the principal allergens in peanuts. The letters of the terminology, Ara h, correspond to the genus and species of the peanut plant, Arachis hypogaea, and the number (1, 2, 3, etc.) distinguishes each discrete protein component. In peanut allergy, 5 proteins are associated with clinical reactions of varying severity: Ara h 1, Ara h 2, Ara h 3, Ara h 8, and Ara h 9. Ara h1, Ara h 2, Ara h 3, and Ara h 9 are associated with severe symptoms whereas Ara h 8 is associated with much milder or no symptoms to peanut. This protein component of peanut is also linked to oral allergy syndrome, also known as pollen-food allergy syndrome. This syndrome is caused by cross-reacting allergens found in both pollen and raw fruits, vegetables, and/or some tree nuts. The immune system recognizes the pollen and similar proteins in the food and directs an allergic response to it. People affected by oral allergy syndrome can usually eat the same fruits or vegetables in a cooked form because the proteins are denatured during the heating process, and the immune system no longer recognizes the food. Palforzia will come packaged in pull-apart capsules or sachets, to be mixed into age-appropriate foods such as applesauce or pudding.
The manufacturer is seeking FDA approval for Palforzia for use only in children between 4 and 17 years of age. In the clinical trials, the starting dose was 0.5 mg. of the product, gradually increasing to a maintenance dose of 600 mg. requiring about 8 biweekly visits to allergist’s office. The new treatment will also likely carry a “black box” warning about possible anaphylaxis and a requirement to carry a self-injectable epinephrine device at all times.
It is likely that patients will need to continue therapy indefinitely, particularly in light of a recent study published online in Lancet on September 13, 2019. The study found that, in patients treated to a point where they could eat peanuts without incident, withdrawal of treatment led to waning tolerance over time. This implies that treatment may be life-long.
The board certified allergists at Black & Kletz Allergy have been diagnosing and treating food allergies for over 50 years. This new medication to treat peanut allergy is exciting and very promising. If this new medication is a success, we feel that there will be other drugs containing other food allergens such as fish, shellfish, milk, egg, wheat, and soy. This is of course pure speculation at this time, but it would make sense to develop other food-related OIT protocols, if Palforzia is successful.
The allergy doctors at Black & Kletz Allergy treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. You may also click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been a fixture in the greater Washington, DC, Northern Virginia, and Maryland metropolitan community for over 5 decades for our outstanding services for the diagnosis and treatment of allergic, asthmatic, and immunological conditions.
Hives (i.e., urticaria) is a type of skin rash that usually presents with red, raised, and itchy bumps, usually similar in appearance to mosquito bites. Other colloquial terms for hives include welts or wheals. They may occur anywhere on the body and appear in various shapes and sizes. They usually blanch with pressure. In some instances, they may look like small red dots or even be flush with the skin. The borders of each hive may be sharply demarcated or they may blend in with the surrounding skin. If the hives are deep enough in the skin layer, the result may be swelling of that area commonly referred to as angioedema.
Hives are quite common as they affect 20% to 25% of the population at some point in their lives. Hives generally, as a rule, are intermittent and usually last less than 24 hours in duration. They may occur very frequently (i.e., multiple times per day) or they may occur very rarely (i.e., one isolated episode). If an episode of hives resolves within 6 weeks, it is known as “acute urticaria.” If the episode lasts more than 6 weeks in duration, it is known as “chronic urticaria.” You may be asking yourself, what are the causes of hives, since they are so common. Many times, the cause is fairly obvious in such cases where the hives develop shortly after eating a certain food, or immediately after a bee sting. They may occur during the course of or shortly after completing a course of antibiotics. Other medications may be the causative agent in others affected with hives. Aspirin and nonsteroidal anti-inflammatory drugs (NSAID’s) are the most common classes of medications that cause hives besides antibiotics. Some of the most commonly prescribed NSAID’s include ibuprofen (Motrin, Advil), naproxen (Aleve, Naprosyn, Anaprox), salsalate (Disalcid), indomethacin (Indocin), etodolac (Lodine), diclofenac (Voltaren, Arthrotec, Cataflam), ketorolac (Toradol), piroxicam (Feldene), meloxicam (Mobic), Oxaprozin (Daypro), nabumetone (Relafen), tolmetin (Tolectin), fenoprofen (Asaid), sulindac (Clinoril), and celecoxib (Celebrex). It is important to note that any medication or food can cause hives in any individual, despite the fact that they may have ingested the food or medication in the past without reactions. An assortment of other conditions such as infections (viral, bacterial, fungal, or parasitic), inflammatory conditions, autoimmune disorders (when the immune system fights an individual’s own tissues and organs instead of defending them against outside intruders), and rarely even cancers can play a role in causing hives. If the hives persist longer than 24 hours and/or they leave residual marks on the skin, it may indicate inflammation of the small blood vessels, a condition known as “vasculitis.” Other factors that may cause or exacerbate hives may include exercise, cold, heat, vibration, pressure, sun exposure, and/or water, to name a few.
If you suffer from hives, it is important to see a board certified allergist such as the allergists at Black & Kletz Allergy. Our allergy specialists see numerous cases of hives and/or swelling episodes each week. We have over 5 decades of experience in the Washington, DC, Northern Virginia, and Maryland metropolitan area in diagnosing and treating hives. We see patients of all ages ranging from newborns to the elderly. At your first consultation with our allergists, a comprehensive history and physical examination will be performed. Depending upon your history and examination, diagnostic tests may include bloodwork, allergy skin testing, urinalysis, X-rays, and/or a skin biopsy. Since histamine is the principal chemical that is responsible for the development of hives, most of the cases are responsive to medications that block the action of histamine on the skin. In some individuals, avoidance of a particular food or medication is all that is needed. For others, there are a variety of treatment options, some of which include antihistamines, leukotriene antagonists, histamine-2 blockers, corticosteroids, immune modulators, and “biologicals” or various combinations of the aforementioned medications.
Black &Kletz Allergy has 3 convenient locations in the Washington, DC metro area. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA which all offer on-site parking. The Washington, DC and McLean, VA locations are Metro accessible and there is a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. Please call us to make an appointment or you can click Request an Appointment and we will reply within 24 hours by the next business day. The allergy specialists of Black & Kletz Allergy are eager to help you with your hives, swelling episodes, allergic rhinitis (i.e., hay fever), asthma, sinus conditions, and immunology needs. We are dedicated to providing excellent care to you as we have been doing in the Washington, DC metro area for more than 50 years.
Proton pump inhibitors (PPIs) are a group of medications commonly used to treat symptoms caused by excessive stomach acid. The most common PPIs available in the U.S. are Nexium (i.e., esomeprazole), Protonix (i.e., pantoprazole), Prilosec (i.e., omeprazole), Prevacid (i.e., lansoprazole), Aciphex (i.e., rabeprazole), and Dexilant (i.e., dexlansoprazole). These medications act by reducing the amount of acid secretion produced by the parietal cells in the lining of the stomach. In addition to lifestyle and dietary modifications, they are usually the first line medications prescribed to treat common conditions such as gastroesophageal reflux disease (GERD), eosinophilic esophagitis (EoE), erosive esophagitis, Zollinger-Ellison syndrome, and peptic ulcers (duodenal or stomach ulcers). GERD is commonly referred to as “heartburn” by the general public. These PPIs are also used in combination with corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), and/or some antibiotics to protect the stomach.
These medications are considered relatively safe and some are also available over the counter. Even though they are available over the counter, there are side effects, particularly if used long-term. Some of the more common side effects may include headaches, rashes, fever, abdominal pain, nausea, vomiting, diarrhea, constipation, lightheadedness, and change in or unpleasant taste. Long-term use has been linked to osteoporosis (i.e., thinning of the bones) which may lead to bone fractures. Other more severe side effects may include acute interstitial nephritis (i.e., kidney failure), lupus, pneumonia, low magnesium levels, muscle spasms, heart palpitations, and clostridium difficile-associated diarrhea, to name a few.
In addition to the side effects of PPIs, there have been a few recent publications that have reported their association with possible allergic reactions.
In an article published in The Journal of Allergy and Clinical Immunology: In Practice,the authors reported serious allergic reactions in five patients receiving PPIs. These patients developed allergic reactions within 30 to 60 minutes of taking the medications orally. One patient developed a more rapid reaction after receiving the drug intravenously.
All patients were subsequently evaluated for sensitivity to PPIs using skin prick testing and intradermal skin testing techniques. All patients showed positive reactions indicating an immediate allergic sensitivity that was mediated by the IgE antibody.
When patients develop life-threatening anaphylactic reactions, foods and insect stings are usually thought to be the causative agents as medications other than penicillins cause anaphylaxis very rarely. However, this report highlights the need for a high index of suspicion for medications such as PPIs being the culprits in causes of anaphylaxis.
A more recent publication in the journal Nature Communications, the authors reported an increase in allergic symptoms in patients receiving PPIs on a regular basis. The data revealed that people taking PPIs for any reason had a two-to-three times higher chance of receiving prescriptions for medications used to treat allergies at a later date.
Stomach acid is needed for proper digestion of ingested food. It contains various enzymes which help break down the complex proteins in the food before they are further processed. It also protects the digestive system from infections caused by bacteria and other harmful substances.
Reducing the acid production by PPIs can impede the proper digestion of proteins. PPIs also alter the microbiome of the stomach. Consequently harmful proteins and other substances can get absorbed into the bloodstream unchallenged. This has the potential to weaken the natural defense mechanisms and can either cause or aggravate allergic sensitization to certain foods and environmental triggers.
The authors of this publication caution people not to use acid suppressor medications any longer than absolutely necessary.
The board certified allergists at Black & Kletz Allergy have 3 convenient locations in the Washington, DC, Northern Virginia, and Maryland metropolitan region and have been providing allergy and asthma care to this area for more than 5 decades. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our offices offer on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. In addition, our McLean, VA office location offers a complementary shuttle that runs between this office and the Spring Hill metro station on the silver line. For an appointment, please call one of our offices. Alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you suffer from allergies or asthma, it is our mission to help alleviate your unwanted symptoms, so that you can enjoy a better quality of life.
Black & Kletz Allergy is dedicated to providing the highest quality allergy and asthma care in a compassionate, relaxed, and professional environment.
Air pollution is a major problem in many parts of the world particularly in major cities in the U.S. including Washington, DC. Air pollution occurs when excessive amounts of gases and/or particles reach harmful levels. It can occur both outdoors as well as indoors. When it is indoors in the workplace, it is often referred to as “sick building syndrome.” Sick building causes are frequently due to failings in the air conditioning, heating, and/or ventilation systems. Other reasons have been attributed to pollutants produced by volatile organic compounds (VOC’s), molds, outgassing of some types of building materials, ozone, lack of adequate filtration or fresh air, and/or chemicals used within a building.
Outdoor air pollution is caused by a multitude of gases, chemicals, and particulates. Carbon dioxide is a known gas which is usually a result of burning fossil fuels such as gasoline, natural gas, and coal. The carbon dioxide in the air causes heat to be trapped in the earth’s atmosphere which is known as the “greenhouse effect.” Many scientists feel that this greenhouse effect can lead to global warming. Another greenhouse gas is methane, which may come from gas emitted by livestock, landfills, and the natural gas industry. Chlorofluorocarbons (CFC’s) are another type of greenhouse gas. They were used in aerosol propellants and refrigerants until the 1980’s when they were banned because of they contributed to the breaking down of the Earth’s ozone layer. Other causes of outdoor pollution include sulfur dioxide and particulates. It should be noted that sulfur dioxide is a component of smog and is the primary cause of acid rain. Smog is a visible form of air pollution and is composed of sulfur oxides (e.g., sulfur dioxide), ozone, nitrogen oxides, smoke and other particulates. Smog is usually thought of to be a summer phenomenon. During the summer when the temperatures are warmer and there is more sunlight present, a photochemical reaction of sunlight, nitrogen oxides, and volatile organic compounds (VOC’s) occurs which produces ground-level ozone that is visible. It looks like smoke and in fact, the word “smog” is a combination of the two words “smoke” and “fog.”
Similar to how allergy sufferers monitor the pollen count, individuals interested in monitoring air pollution can follow the air quality index (AQI). The higher the AQI number, the greater the level of air pollution, and thus the greater the health concern. The AQI ranges from 0 to 500 whereby levels between 151 and 500 are “unhealthy.” An AQI number between 0 and 100 is considered to be acceptable by the Environmental Protection Agency (EPA). An AQI value between 101 and 150 may be unhealthy for sensitive (e.g., allergy sufferers, asthmatics, people with other lung diseases and/or heart disease, the elderly, children) individuals. An AQI value of over 300 is hazardous to one’s health. The EPA has assigned a color with each designated specific range of the AQI. The level of health concern, AQI values and colors (e.g., green, yellow, orange, red, purple, maroon), and their meaning are as follows:
Air Quality Index (AQI) ValuesLevels of Health ConcernColorsWhen the AQI is in this range:..air quality conditions are:…as symbolized by this color:
0 to 50
Good
Green
51 to 100
Moderate
Yellow
101 to 150
Unhealthy for Sensitive Groups
Orange
151 to 200
Unhealthy
Red
201 to 300
Very Unhealthy
Purple
301 to 500
Hazardous
Maroon
Note: Values above 500 are considered Beyond the AQI. Follow recommendations for the Hazardous category. Additional information on reducing exposure to extremely high levels of particle pollution is available here.
Individuals with allergies and asthma are generally more susceptible to the side effects of air pollution. In many cases the particulates, gases, and chemicals can trigger asthma and/or incite nasal and eyes symptoms consistent with allergic rhinitis and allergic conjunctivitis. Others are affected by air pollution as a direct irritant-type nonallergic reaction. The most common symptoms caused by air pollution may include irritated eyes, burning of the eyes, red eyes, watery eyes, runny nose, burning of the nose, sore throat, fatigue, headaches, coughing chest tightness, chest pain, and/or shortness of breath.
There are some preventive measures as well as recommended treatments that should be undertaken when the AQI values rise. In consultation with one of our board certified allergists at Black & Kletz Allergy, we discuss these issues as well as others in order to prevent untoward and unnecessary reactions to all types of pollution.
The allergists at Black & Kletz Allergy have been diagnosing and treating allergies, asthma, sinus conditions, and immunological disorders for more than 50 years. We have been a proponent of a clean environment for a long time and Dr. Kletz has done volunteer work for the American Lung Association. Black & Kletz Allergy has 3 convenient locations in the Washington, DC metro area with offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. We offer on-site parking at each location and the Washington, DC and McLean offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. Please call us today to make an appointment at the office of your choice. Alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. The allergists at Black & Kletz Allergy pride themselves in the delivery of the highest quality allergy care in the Washington, DC metropolitan area. In addition, we strive to provide excellent customer service in a friendly and affable environment.
In the hectic days we live in, many individuals feel fatigued or exhausted. Fatigue is a very common symptom that can be either chronic or intermittent. Many people seek help by seeing a physician in order to find out the cause of their fatigue, as there are many potential causes. Despite the numerous causes of fatigue, underlying allergies is a fairly common reason for fatigue in many individuals.
Usually patients with allergic rhinitis (i.e., hay fever) and allergic conjunctivitis exhibit many of the classic symptoms of allergies which may include sneezing, runny nose, nasal congestion, post-nasal drip, itchy nose, itchy throat, itchy ears, clogged ears, itchy eyes, watery eyes, redness of the eyes, puffy eyes, sinus pressure, and/or sinus headaches. The typical symptoms in individuals with asthma may include wheezing, chest tightness, shortness of breath, and/or coughing. It should also be noted that food allergies can cause fatigue in certain individuals in addition to the more typical abdominal symptoms (e.g., abdominal pain, diarrhea), skin symptoms (e.g., hives, itching, swelling), lung symptoms (e.g., wheezing, shortness of breath, coughing), and of course anaphylaxis. Even though the symptoms listed above are the “more typical” symptoms associated with allergies, asthma, and food allergies one should realize that fatigue is not an uncommon symptom that occurs in allergic individuals. There are in fact people that only complain of fatigue and do not have any of the more typical symptoms of allergies. You may be asking: How do you know if your fatigue is due to allergies? It should be noted that there are a whole host of conditions and/or reasons that can cause fatigue. Likewise, it is important to rule out these “other” causes of fatigue before declaring one’s fatigue is due to allergies.
What are some common causes of fatigue besides allergies? Here are some of the more common reasons/conditions that may cause fatigue, but keep in mind that there are numerous other conditions or reasons that may cause fatigue that are not listed below:
Fatigue Can Be Due to Allergies?Assuming that there are no other reasons for one’s fatigue, seeing a board certified allergist in the Washington, DC, Northern Virginia, and Maryland metropolitan area is important in order to rule out allergies as a cause. In fact, even if you have another condition that can cause fatigue, it is still possible that some or all of your fatigue may be coming from allergies. The board certified allergists at Black & Kletz Allergy are experts in the field and can find out if you have allergies via blood and/or skin testing. It is first important for the allergist to perform a comprehensive history and physical examination. Allergy testing is done in order to identify if, what, and how allergic one is to specific allergens. Once an allergy is identified, preventive measures are discussed in order to minimize one’s exposure to the offending allergens. In addition, the use of allergy medications are usually beneficial in alleviating those unwanted allergy symptoms which also includes fatigue. Allergy immunotherapy (i.e., allergy shots, allergy injections, allergy hyposensitization) may be utilized to treat the underlying allergies as they are very efficacious and are beneficial in 80-85% of individuals who take them. Most individuals are on allergy shot for 3-5 years.
The allergists at Black & Kletz Allergy see both pediatric and adult patients and have over 50 years of experience in the field of allergy, asthma, and immunology. Black & Kletz Allergy has 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call any of our offices or you may click Request an Appointment and we will respond within 24 hours by the next business day. We have been servicing the greater Washington, DC metropolitan area for over 5 decades and we look forward to providing you with the highest state-of-the-art allergy care in a friendly and comfortable environment.
If you are like a lot of individuals in the Washington, DC, Northern Virginia, and Maryland metropolitan area, then you may suffer from allergies. There is an old adage that says that if you move to the Washington, DC area and you do not have allergies, you eventually will! This is not true of course, however, many individuals in the area (whether or not they grew up or moved to the Washington, DC area) do in fact have allergies, particularly allergic rhinitis (i.e., hay fever).
The classic symptoms of allergic rhinitis as well as non-allergic rhinitis may include any or all of the following: nasal congestion, runny nose, post-nasal drip, itchy nose, sneezing, itchy throat, itchy eyes, watery eyes, red eyes, puffy eyes, snoring, fatigue, sinus congestion, headaches, and dark circles under the eyes. Allergies commonly trigger asthma as well. Affected individuals may experience chest tightness, wheezing, coughing, and/or shortness of breath.
It should also be noted that allergies increase the risk of sinus disease, sinus infections, and nasal polyps. Sinus infections can be categorized into 3 distinct types: acute, chronic, and recurrent. It is important for the allergist to be able to distinguish between the three, as the treatment is different for each type. Acute sinusitis: This type of sinus infection is the most common of the three types and often presents with nasal congestion, sinus pressure and/or pain which can radiate to the teeth, discolored nasal discharge, and a post-nasal drip. Occasionally, a fever may be present in some individuals with acute sinusitis. The diagnosis is usually made by a detailed history and a physical examination. Treatment may necessitate the use of antibiotics, nasal corticosteroids, saline irrigation of the nose, and/or decongestants. Rarely, it may be beneficial to use oral corticosteroids is severe cases.
Chronic sinusitis: The common manifestations of a chronic sinus infection generally include nasal congestion, facial pressure/pain, headache, discolored nasal discharge, post-nasal drip, cough, loss of taste and smell, and/or malaise. The diagnosis requires a comprehensive history of onset and progression of specific symptoms, a detailed physical examination, and imaging studies such as CT scans and/or sinus X-rays. The management of chronic sinusitis usually entails a prolonged course (e.g., 30 days) of antibiotics in addition to nasal corticosteroids, saline irrigation of the nose, and/or decongestants. It may be necessary to give another prolonged course of antibiotics in recalcitrant cases. Surgical intervention may also be necessary if medical therapy is unsuccessful. It is important to note that some individuals may only present with chronic nasal congestion as their only symptom.
Recurrent sinusitis: This type of sinus condition is merely repetitive acute sinus infections. Individuals that get repeated episodes of acute sinusitis may have an immune disorder or a weakened immune system. It is thus important to see a board certified allergist/immunologist like the ones at Black & Kletz Allergy. Blood tests to assess a patient’s immune system are often ordered in individuals who suffer from recurrent sinusitis in order to rule out or diagnose an immune defect. Patients who are found to have an immunodeficiency are then treated with appropriate therapy depending upon their specific immune defect. In addition, the sinus infection is treated with antibiotics, topical nasal corticosteroids, saline irrigation of the nose, and/or decongestants.
The prevention of sinusitis includes identification of specific allergen sensitivities by allergy testing by a board certified allergist. Allergy testing may be done by skin testing or blood testing depending upon the circumstance and age of the patient. The aggressive treatment of allergic seasonal and/or perennial rhinitis (i.e., hay fever) promotes proper sinus drainage and improves upper airway function.
Therapies used to treat allergic rhinitis may include antihistamines, nasal corticosteroids, nasal antihistamines, saline irrigation of the nose, decongestants, leukotriene antagonists, and/or allergy immunotherapy(i.e., allergy shots, allergy injections, allergy desensitization, allergy hyposensitization). Allergy shots are effective in 80-85% of patients who take them. They have been used in the U.S. for more than 100 years and are used in both children and adults.
The board certified allergists at Black & Kletz Allergy have been diagnosing and treating sinusitis for more than 50 years. We treat both adult and pediatric patients. Black & Kletz Allergy has offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. Our McLean office location offers a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you suffer from allergies and/or sinus-related symptoms, we are here to help alleviate or hopefully end these undesirable symptoms that have been so troublesome, so that you can enjoy a better quality of life. Black & Kletz Allergy is dedicated to providing the highest quality allergy care in a relaxed, caring, and professional environment.
Coughing is a protective “reflex” given to us by nature as part of our body’s vital defense mechanisms. It forcibly expels harmful bacteria, viruses, foreign objects, and excessive mucus from the respiratory tract protecting our lungs from irritation, inflammation, and infections.
Mechanism:
There are 4 stages in a cough reflex:
An initial deep inspiration filling the lungs with air.
Closure of epiglottis .
Forcible contraction of the muscles of the chest and abdomen which pushes up the diaphragm causing compression of the lungs.
As the pressure builds up, the epiglottis is forced open allowing the air to rush out at a high speed producing a whooping noise.
Coughing can be a voluntary act, conscious action, or more commonly an involuntary uncontrollable process. The reflex is initiated by stimulation of the nerve fibers in the respiratory tract by various substances such as smoke, cold air, allergens, microbes, and tumors, as well as from irritation by normal secretions such as mucus and/or stomach acid.
All of us cough from time to time. It is very common during colds (i.e., upper respiratory infections), which are usually viral in nature. Coughing also is common during acute bronchitis and pneumonia (i.e., lower respiratory infections involving mainly the lungs). It should be noted that following infections, a cough may linger for a few weeks before it subsides.
A cough that lasts for months (and sometimes years) is described as “chronic” and is one of the most common reasons why healthcare providers are consulted. A cough may interrupt sleep resulting in daytime somnolence and affect school and work performance. Vigorous coughing may also cause physical effects such as urinary incontinence and rib fractures.
Causes:
Smoking: Most cigarette smokers eventually develop a “smoker’s cough”. Irritation by noxious chemicals is the predominant cause. Smoke also plays a significant role in causing chronic bronchitis, emphysema, and lung cancer.
Post-nasal Drip: In addition to aiding in the perception of smell, the nose also protects the lungs by filtering, warming, and humidifying the air entering the lower respiratory tract. It accomplishes this by secreting warm, moist, and sticky mucus. When the nose is irritated by chemicals, allergens, microbial organisms, etc., it secretes excessive mucus which is usually thin and watery. When these copious secretions run down the back of the throat, they irritate the nerves in that area, cause a tickling sensation which may trigger a cough reflex. A post-nasal drip can often be controlled by avoiding exposure to known triggers and stimuli. Medications such as antihistamines, decongestants, and nasal sprays may help relieve the cough caused by a postnasal drip. Home remedies such as steam inhalation and saline nasal irrigation also may play a role in treatment.
Asthma: Chest tightness, wheezing, and shortness of breath usually accompany cough in individuals with asthma. However, in a variant of this condition, a cough may be the only presenting manifestation. This is called cough variant asthma. The diagnosis is established by pulmonary function testing (sometimes after inhalation of a chemical (e.g., methacholine) that can trigger symptoms which can then be relieved by a medication that opens up the airways). Occasionally, a therapeutic trial of anti-inflammatory inhaled medications (i.e., inhaled corticosteroids) on a regular basis for a few weeks is helpful in arriving at the diagnosis.
Gastroesophageal Reflux Disease (GERD): When stomach acid travels up the food pipe (i.e., esophagus), it usually causes heartburn, belching, sore throat, and/or hoarseness. However, in one third of patients it manifests only as a chronic cough without the other symptoms. Confirmation of the diagnosis is established by placing a probe in the esophagus and monitoring the pH for acidity for 24 hours. A simpler approach is to empirically treat the individual with lifestyle modifications (e.g., avoiding alcohol, spicy foods, citrus fruits, bulky meals, and carbonated beverages). If the symptoms persist, medications to neutralize the acid and/or reduce acid secretion may be utilized.
Chronic Bronchitis: Prolonged inflammation of the tissues in the lungs from chemical irritants and pollutants can cause a chronic cough. Imaging studies are sometimes needed to rule out anatomical and structural abnormalities. Some patients may need long term anti-inflammatory inhaled medications (e.g., inhaled corticosteroids) to control a chronic cough.
ACE inhibitors: These medications are often used to treat high blood pressure and/or heart failure. Up to 20% of people receiving these medications may develop a cough after a few weeks, which is a known side effect of these types of medications. They may need to discontinue these medications and begin taking an alternative medication in order to get relief from their cough.
Heart Disease: Congestive heart failure can cause either a dry cough or a productive cough associated with a frothy, thin, white sputum. Leg swelling (i.e., edema), fatigue, and exercise intolerance are other common symptoms of congestive heart failure.
Aspiration: When food finds its way into windpipe (i.e., trachea) instead of food pipe (i.e., esophagus), it triggers a recurrent cough. This is more common in patients with strokes and other chronic neurological disorders.
Lung Cancer: It is a rare cause of chronic cough in non-smokers, and more common in smokers.
Stress: “Psychogenic” coughing increases at times of stress and usually disappears or diminishes during sleep.
Chronic sinusitis: It is fairly common for individuals with a chronic sinus infection (i.e., chronic sinusitis) to experience a chronic cough. In some cases, it is the only symptom of their sinus condition. In others, it may be accompanied by symptoms such as nasal congestion, decreased ability to smell and/or taste, post-nasal drip, discolored nasal discharge, sinus pressure, and/or sinus headaches.
Cough Medications:
Dextromethorphan is a commonly used, partially effective cough suppressant. Prescription medications containing codeine and its derivatives are more effective but have more undesirable side effects and may be habit-forming.
Guaifenesin is the most commonly used expectorant which may be useful in thinning out viscous secretions which ultimately help the mucus drain more easily.
Warning Signs: One should consult his or her physician as soon as possible if one experiences any of the following symptoms: bloody sputum, fever, weight loss, night sweats, breathlessness, excessive fatigue, and/or chest pain.
The board certified allergy doctors at Black & Kletz Allergy have a great deal of experience in diagnosing and treating both adults and children with a chronic cough. It is important to find the underlying reason for a cough in order to treat it appropriately. At Black & Kletz Allergy, we search for a cause beginning with a comprehensive history and physical examination. Breathing tests, X-rays, blood tests, and/or allergy skin tests may be performed depending upon each individual’s history and physical, as it is tailored to each person’s own situation.
The allergists at Black & Kletz Allergy have 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. Our Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call one of our offices or alternatively, you may click Request an Appointment and we will respond within 24 hours by the next business day. We have been servicing the greater Washington, DC area for more than 50 years and we look forward to providing you with excellent state of the art allergy care in a welcoming and professional environment.
Symptoms such as nasal congestion, clear runny nose, and itchy throat are most commonly due to sensitivity to common “allergens” in the environment (e.g., pollens, dust mites, mold spores, animals). Our immune system mistakes them as potentially harmful and thus mounts a defensive attack on these substances when it encounters them. During this process, there is a release of chemical substances (e.g., histamine, prostaglandins, leukotrienes) into the tissues inside the nose and eyes and these chemicals are responsible for the symptoms of allergies.
The symptoms may be relieved with medications that block the actions of these chemicals which can be utilized to make allergic individuals more comfortable. The symptoms may also be prevented either by avoiding the exposure to the allergens, by environmental controls, or by getting desensitized to the allergens by allergy immunotherapy (allergy shots, allergy injections, allergy desensitization, allergy hyposensitization). Sensitizing allergens can vary from person to person and allergy tests obtained by skin or blood testing are needed to identify the offending allergen in order to consider specific environmental controls and/or desensitizing treatments.
What if one has all the symptoms suggestive of “allergies” but all the tests are negative? You may have a condition called vasomotor rhinitis or more appropriately called non-allergic rhinitis.
The symptoms of non-allergic rhinitis may include:
Nasal congestion
Runny nose
Sneezing
Mucus (i.e., phlegm) in the throat (e.g. post-nasal drip)
Cough
These symptoms can be long term or may last only a short period of time. They can come and go all year-round. Itching of the nose, eyes, and/or throat are not present in non-allergic rhinitis as they are more likely to be features of allergic rhinitis (i.e., hay fever).
The exact cause of non-allergic rhinitis is not known. The effect is widening of the blood vessels inside the nostrils and leakage of fluids into the tissues resulting in excessive mucus and swelling of the mucus membrane linings and nasal turbinates.
The common triggers of non-allergic rhinitis are:
Environmental or occupational irritants: Dust, smoke, pollutants, strong odors, perfumes, colognes, potpourri, chemical sprays, fumes, etc.
Weather changes: Fluctuations in temperature and humidity.
Food: Hot and spicy foods, certain alcoholic beverages.
Infections: Viral infections such as the common cold or influenza (i.e., the flu)
Medications: Aspirin, Ibuprofen, certain blood pressure medications (e.g., beta-blockers ACE inhibitors), sedatives, antidepressants, and oral contraceptives.
Rhinitis medicamentosa: Prolonged and/or overuse of over-the-counter decongestant nasal sprays (e.g., Afrin, Neosynephrine) can cause rebound congestion and habituation.
Hormonal changes: Pregnancy, menstruation, and hypothyroidism.
Stress: Emotional or physical stress.
Other triggers: Sleeping posture, sleep apnea, acid reflux, etc.
Complications:
Nasal polyps: These are soft, benign growths that develop on the lining of the nose or sinuses due to chronic inflammation. Small polyps may not cause problems, but larger ones may block the airflow through the nose, making it difficult to breathe. They also increase the likelihood of recurrent sinus infections.
Sinusitis: Prolonged nasal congestion due to non-allergic rhinitis may increase the chances of developing sinusitis, an infection or inflammation of the membranes that line the sinuses.
Middle ear infections: Increased fluid and nasal congestion may lead to middle ear infections.
Interrupted daily activities: Non-allergic rhinitis may affect focus and concentration and in turn impact learning at school and/or productivity at work.
The diagnosis is established when one presents with the classic symptoms of rhinitis and when the skin tests and/or blood tests fail to identify specific environmental sensitivities. Common infections of the nose and sinuses also need to be ruled out by examination and imaging tests. There are no confirmatory tests for non-allergic rhinitis and it is usually an exclusion diagnosis.
Treatment:
Avoidance of the common triggers is the first step in the management of non-allergic rhinitis. When avoidance is not possible or when it does not work, the following actions may be helpful.
An over-the-counter nasal saline spray or homemade salt water solution to flush the nose of irritants and help thin the mucus and soothe the membranes inside the nose.
Corticosteroid nasal sprays (e.g., fluticasone, triamcinolone, budesonide) may help reduce the congestion due to their anti-inflammatory effect by shrinking the swelling and reducing excessive mucus production.
Antihistamine nasal sprays (e.g., azelastine, olopatadine) are more helpful than oral antihistamines in relieving the symptoms of non-allergic rhinitis.
Anticholinergic nasal sprays (e.g., ipratropium bromide) can help to dry up the excessive nasal secretions and relieve runny nose and post nasal drip.
Oral decongestants (e.g., pseudoephedrine, phenylephrine) can help relieve nasal stuffiness by shrinking the blood vessels and reducing mucus buildup. Side effects of these medications however may include elevated blood pressure, rapid pulse, restlessness, sleep disturbances, palpitations, and/or tremors.
Prevention:
A recent small study showed that eating oily fish (e.g., herring, mackerel, salmon) at least once a week may reduce the risk of rhinitis. However more studies are needed to confirm this finding.
The board certified allergists at Black & Kletz Allergy have 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. The allergy specialists at Black & Kletz Allergy are extremely knowledgeable regarding non-allergic rhinitis as well as allergic rhinitis. We diagnose and treat both pediatric and adult patients. In addition, we treat patients with food, medication, insect sting, and skin allergies, asthma, eosinophilic esophagitis, sinus disease, and immunological disorders. To schedule an appointment, please call any of our offices or you may alternatively click Request an Appointment and we will respond within 24 hours by the next business day. We have been servicing the Washington, DC, Northern Virginia, and Maryland metropolitan area for more than 50 years and we look forward to providing you with comprehensive state-of the-art allergy care in a friendly and professional environment.
Does eating local honey help treat allergies? This question has been asked for decades. Many individuals swear that consuming local honey does help alleviate their seasonal allergy symptoms known as allergic rhinitis (i.e., hay fever). Beekeepers generally also agree with this theory. In order to answer this question, another important question to ask is “how does local honey help allergies?”, if in fact it does help.
The theory behind this hypothesis is rooted in the fact that when bees land on flowering trees and plants, the pollens that are on the flowers stick to the bees’ abdomens. When bees make honey, the pollen that is on their abdomen is incorporated in the honey. Local honey contains the pollen of these flowering trees and plants. Processed honey that you would typically buy at a grocery store is usually micro-filtered and pasteurized. These processes generally remove the pollen from the honey. The thought is that local “raw” honey contains pollens from local trees and plants and by eating the honey, an individual will develop a “resistance” to the pollens that are in the local honey. This would then lead to less or no allergic symptoms when exposed to these local pollens. In theory, this sounds good, but in fact, there are flaws in this concept which are as follows:
The first fault in this idea is that individuals suffering from seasonal allergies in the Spring are allergic to non-flowering trees such as maple, birch, elm, hickory, cedar, ash, beech, and oak trees. They are not generally allergic to the pollen from flowering trees and plants such as cherry trees, Bradford pear trees, redbud trees, dogwood trees, and forsythia bushes. The reason for this is fairly simple. The pollen of flowering trees and plants are heavy in weight and thus are not wind-dispersed. Since the pollen is heavy, through evolution, these types of trees and plants had to develop flowers in order to attract bees so that they could cross-pollinate and thus reproduce. The bees land on a flower and the pollen then sticks on the abdomen of the bees. The bees then fly to another same species flowering tree or plant and when they land on these flowers, the pollen on their abdomen gets distributed on this new flower and hence cross-pollination occurs. The fact that the pollen is heavy and not wind-dispersed means that individuals do not inhale the pollen and therefore do not become sensitized or allergic to these pollens. Unlike flowering trees and plants, the non-flowering tree pollens are light in weight and are wind-dispersed, thus able to cause sensitization and allergy symptoms to allergic-prone individuals. This translates into the fact that eating local honey (which is composed of flowering tree pollens) will not reduce one’s allergies in the Spring because it does not contain the correct types of pollens that cause hay fever.
In addition, the amount of pollen in local honey is not consistent between different bottles of honey from the same beekeeper yet from different beekeepers. It is not standardized. The idea of allergen desensitization (i.e., allergy immunotherapy, allergy hyposensitization) is to give a very low tolerable dose and increase the amount slowly over time, so that an individual can become tolerant to that allergen (e.g., tree pollen).
Another major flaw in this theory is that there have been no good scientific studies showing any advantage in using local honey to treat allergies. There are a few studies that are flawed in the manner the studies were done as well as the number of participants are too small to make a general correlation between consuming local honey and its effects on allergies. The use of honey to treat allergies is also not endorsed by either the American Academy of Allergy, Asthma & Immunology or the American College of Allergy, Asthma & Immunology.
Honey does have some advantages however. It is not uncommonly used to help alleviate coughs and of course, it tastes good! It is also interesting to point out that honey does not spoil. This is thought to occur because organisms cannot survive long enough within a jar of honey due to the very low moisture that exists in a jar of honey and thus does not have the chance to spoil.
All in all, honey has its merits, but treating allergies is not one of them. If you suffer from allergies, please contact Black & Kletz Allergy so that you can see one of our board certified allergists in the Washington, DC, Northern Virginia, and Maryland metropolitan area. After a comprehensive history and physical examination, allergy testing may be done and the appropriate avoidance measures will be discussed. Depending upon each individual’s results, medications and/or allergy shots (i.e., allergy immunotherapy) may be prescribed. Allergy shots have been prove to be effective in 80-85% of patients undergoing injections and they have been given in the United States for over 100 years. Unlike consuming local honey, there are numerous studies demonstrating the efficacy and benefits of allergy immunotherapy when administered in the proper way.
The allergy doctors at Black & Kletz Allergy treat both adult and pediatric patients. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of the offices have on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and the McLean, VA office has a free shuttle that runs between our office and the Spring Hill metro station on the silver line. You may also click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been a fixture in the greater Washington, DC and Northern Virginia community for over 50 years for our exceptional services for the diagnosis and treatment of allergic, asthmatic, and immunological conditions.
Eczema (i.e., atopic dermatitis) is a genetically determined condition which causes long term inflammation of the skin which may result in itching, thickening, redness, and occasionally ulcerations of the skin. A similar appearance can sometimes be seen in other chronic skin conditions.
Eczema or atopic dermatitis affects an estimated 7% of the population with varying degrees of severity. It often begins in early childhood and may wax and wane throughout a lifetime. The severity can vary from mild dryness and/or excessive creasing of the skin to a severe debilitating illness presenting with painful sores and/or skin infections. The intractable itching often does not respond to medications and may lead to loss of sleep, inability to focus on work and/or school, and/or emotional problems.
Unfortunately there is no known cure for the condition yet. The flare-ups of this disorder are typically treated with topical and/or oral corticosteroid medications, which usually offer only short-term relief. The numerous topical corticosteroids available vary in potency and should be prescribed based on the severity of the eczema as well as the location of the eczema on the body. The side effects of the corticosteroid medications can also be worrisome, so it is important to use them sparingly and to avoid excessive use. A few new non-steroidal topical medications and injectable biological medications have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of atopic dermatitis. It is important to note that the response rates to these medications are highly variable. There are also side effects one should be aware of regarding the biological medications in particular.
Despite the fact that allergy immunotherapy is so efficacious in allergies of the respiratory tract and eyes, allergy immunotherapy has not been studied extensively in patients with eczema. A case-study, however, presented at a recent annual scientific meeting of the American College of Asthma, Asthma & Immunology, offers hope.
In this case-study, a 48 year-old man who had suffered from severe eczema involving a large part of his body since his childhood was observed. He had tried many therapies for years including both mild and high-strength topical corticosteroid creams, other topical anti-inflammatory creams, and topical moisturizer creams without adequate relief.
Since he also had respiratory allergy-related symptoms, his doctors tested him for environmental allergies and diagnosed him with sensitivity to dust mites, molds, animal dander, trees, grasses, and weeds. In fact allergic rhinitis, asthma and eczema constitute the “atopic triad” and share a similar genetic predisposition.
Because his allergies could all be treated with allergy shots, his doctors thought that treating his allergies may also be beneficial for his eczema. After one year of allergy shots, he reported significant improvement of his eczema symptoms. Once he reached a maintenance dose on his allergy shots, he no longer needed high dose corticosteroid treatment for his eczema.
There is a need for more extensive controlled studies investigating the benefits of allergy shots for individuals with moderate to severe eczema. If further studies substantiate the data observed in this patient, allergy shots have the potential to benefit thousands of people with severe recalcitrant eczema.
The board certified allergists at Black & Kletz Allergy see patients of all ages and have over 50 years of experience in the field of allergy, asthma, and immunology. In addition to allergic rhinitis, allergic conjunctivitis, and asthma, skin disorders such as eczema, contact dermatitis, poison ivy, poison oak, poison sumac, hives (i.e., urticaria), generalized itching (i.e., pruritus) are common skin ailments that we routinely diagnose and treat. Black & Kletz Allergy has 3 offices in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA and all locations have on-site parking. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. To make an appointment, please call us or alternatively, you can click Request an Appointment and we will respond to your request within 24 hours by the next business day. The allergists at Black & Kletz Allergy are happy to answer any questions or concerns you may have about any allergic, asthmatic, or immunologic concern.
The typical hay fever signs and symptoms may include sneezing, runny nose, nasal congestion, post-nasal drip, a horizontal crease at the bottom third of the nose, itchy nose, itchy eyes, watery eyes, redness of the eyes, puffy eyes, dark circles under the eyes, a line or fold in the skin below the lower eyelids, itchy mouth and throat, itchy ears, clogged ears, coughing, itchy skin, and/or sinus pressure. In the Spring in the Washington, DC metro area, the tree and grass pollens as well as molds are generally to blame for these annoying allergy symptoms. In the Fall, ragweed and molds are generally the culprits when it comes to causing hay fever symptoms. Ragweed generally begins to pollinate in mid-August and is typically ends at the first frost which is usually at the end of October.
In asthmatics, the characteristic symptoms that may occur include chest tightness, wheezing, shortness of breath, and/or coughing. The most common allergens that cause an increase of these asthma symptoms include tree pollens in the early Spring, grass pollens in the late Spring, and molds, which occur throughout the Spring. It is important to know that molds are prevalent throughout every month of the year and are present both indoors and outdoors. As mentioned in the paragraph above, ragweed, along with molds are the principle allergens that cause asthma exacerbations in the Fall.
It is interesting to note that there are a variety of other rarer symptoms that some individuals may notice in the Spring and Fall. In fact, these symptoms may be perennial in nature which can be confusing since they can signify other medical conditions. These less common allergy symptoms may include fatigue, “fogginess” feeling of the head, ringing of the ears (i.e., tinnitus), joint achiness, headaches, itchy mouth, abdominal pain, diarrhea, sore throat, behavioral issues (e.g., moodiness, hyperactivity, inability to concentrate), snoring, and/or rashes.
Note that the combination of fatigue, achiness, runny nose, nasal congestion, and sneezing can easily be misconstrued for the common cold. One should be aware that the common cold is caused by a virus, and that in general, “colds” usually last no more than 7-10 days. This means that if an individual is experiencing “cold” symptoms for a long period of time (i.e., greater than 2 weeks) and/or if he or she is experiencing recurrent “cold” symptoms every Spring or Fall, then allergies should be seriously considered and one should make an appointment with a board certified allergist such as the ones at Black & Kletz Allergy.
A few words about some of the less common seasonal allergy symptoms are discussed below:
Fatigue: Usually occurs due to poor quality or quantity of sleep as a result of poorly controlled allergies. In some individuals, this fatigue can be rather severe.
“Fogginess” feeling of the head: May be due to increased sinus pressure.
Ringing of the ears: Usually due to blockage of the Eustachian tube which stems from sinus congestion.
Joint achiness: May be due to inflammation caused by allergies
Headaches: Seasonal allergic headaches are usually due to increased nasal and sinus congestion. They tend to be in the forehead and cheek regions of the face.
Itchy mouth, Abdominal pain, and/or Diarrhea: Some pollen-allergic individuals have a condition called oral allergy syndrome (i.e., pollen-food allergy syndrome) whereby they have a local reaction in the gastrointestinal tract (i.e., mouth, esophagus, stomach) to certain foods (usually fresh fruits and/or vegetables). Usually these individuals will experience an itchy mouth or throat from eating these raw fruits and vegetables, however, sometimes more severe gastrointestinal reactions may occur such as abdominal pain and/or diarrhea. Some common cross-reactive foods and pollens include: birch tree pollen – apples, pears, peaches, celery, carrots; ragweed pollen – melons, bananas, kiwi.
Sore throat: Usually associated with a post-nasal drip but can also be caused by excessive dryness due to the use of antihistamines.
Behavioral issues: Usually die to poor quality or quantity of sleep.
Snoring: Usually due to increased nasal congestion. Note that an increase in nasal congestion may also worsen obstructive sleep apnea and thereby cause an increase in snoring.
Rashes: Seasonal allergies can cause a flare-up of eczema (i.e., atopic dermatitis). Some allergic individuals may develop itching and rashes when they come in direct contact with an allergen such as grass.
The board certified allergy specialists at Black & Kletz Allergy have 3 convenient locations in the Washington, DC metro area. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our offices have on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. Our McLean, VA office location offers a complementary shuttle that runs between this office and the Spring Hill metro station on the silver line. For an appointment, please call one of our offices or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you suffer from allergies or asthma, it is our mission to help alleviate or end your undesirable symptoms, so that you can enjoy a better quality of life. We have been serving the community’s allergy and asthma needs for more than 50 years. Black & Kletz Allergy is dedicated to providing the highest quality allergy care in a caring, relaxed, and professional environment.
The most common cause in the Washington, DC, Northern Virginia, and Maryland metropolitan area for itchy, red eyes in the Spring and Fall high pollen seasons is inflammation of the thin membrane covering the eyeballs (i.e., conjunctivae). This inflammation is triggered by allergen exposure to susceptible individuals. However, inflammation to the conjunctivae can also be caused by infections by microorganisms such as viruses, bacteria, and rarely fungi and parasites.
It is very important for a board certified allergist to distinguish the difference between these two conditions as the treatment options are determined by the causative factors and differ greatly.
Though it is not always possible to differentiate the conditions by symptoms alone, the following information can be a helpful beginning.
If the discharge from the eye(s) is anything more than normal tears, it is more likely to be something more than allergies. Though allergies also can cause much discomfort, pain in the eye(s) is more indicative of an infectious process.
A definitive diagnosis can only be made by examination and testing by trained and experienced professionals.
Allergies are not contagious to others but infections can easily spread from person to person or from one eye to the other eye. The signs and symptoms of eye allergies (i.e., allergic conjunctivitis) are more likely to occur in both eyes, whereas infections are more likely to develop in one eye initially, although both eyes may be affected.
Prevention and Treatment:
Allergic Conjunctivitis:
Prevention should include reducing one’s exposure to known allergens by restricting outdoor activities on high pollen days, keeping windows closed, keeping pets out of the bedrooms, and using air purifiers and dehumidifiers to minimize dust mite and mold growth.
Treatment involves using over-the-counter eye drops containing antihistamines and mast cell stabilizers. These are often helpful in relieving the itching and redness that are characteristic of allergic conjunctivitis. They can be supplemented with oral medications (e.g., antihistamines) especially if nasal and sinus symptoms are also present. Over-the-counter artificial tears also can help keep eyes moistened and flush out allergens. In case of persistent symptoms, certain nasal corticosteroids, but not all, have the indication to help alleviate the allergic eye symptoms that may be extremely bothersome to the allergic individual. Though they are more efficacious, the risks of adverse effects are also higher.
Prevention should entail avoiding exposure to people battling viral and bacterial infections to the best of their ability. In addition, frequent hand washing can reduce the risks of contracting and spreading infectious eye conditions.
The treatment of infectious conjunctivitis varies depending on the microorganism.
Most viral infections resolve after a few days without any specific antiviral medications. Lubricating eye drops and cold compresses can help relieve the discomfort and facilitate recovery.
Bacterial infections need antibiotic eye drops, instilled several times a day for about a week in order to treat the infections. Rarely infections can also be caused by fungi and/or parasites. In these rare cases, anti-fungal and anti-parasitic medications can be administered.
If eye infections are mistakenly self-treated with over-the-counter allergy medications, one can run the risk of damaging the eyes.
Other Ocular Allergies:
Of note, there are 3 other forms of ocular allergies that are more severe than allergic conjunctivitis which include the following:
Vernal keratoconjunctivitis (VKC): A chronic inflammatory swelling of the outer lining of the eyes due to an allergic reaction. It typically affects boys and young males who live in hot dry climates in a seasonal manner, most often occurring in the Spring and/or Summer. It usually occurs in patients with a family history of allergies. The classic symptoms may include watery eyes, itching, redness, and/or increased sensitivity to light (i.e., photophobia) of both eyes. The treatment is similar to that of allergic rhinitis (see below), but in addition, individuals with severe cases may need topical corticosteroids, cyclosporine, or tacrolimus. Rarely, oral corticosteroids may be necessary in recalcitrant cases. It should be noted that rarely, VKC can lead to corneal scarring and vision loss if not properly treated.
Atopic keratoconjunctivitis (AKC): A genetic disorder that is more common in adults (men more than women) where the immune system produces higher amounts of antibodies in response to a given allergen. Although AKC is perennial in nature, the symptoms may worsen in the Winter. Individuals usually have a history of eczema (i.e., atopic dermatitis). The typical symptoms may include red eyelids, burning, itching, watery eyes, and/or increased sensitivity to light (i.e., photophobia) of both eyes. The treatment is similar to that of VKC. It should be noted that rarely, AKC can lead to corneal scarring and vision loss as mentioned above with VKC. This complication however occurs more often in individuals with AKC than with VKC.
Giant papillary conjunctivitis (GPC): A disorder that causes inflammation in the inside part of the eyelid. It is most often caused by a reaction to eyelid movement over a foreign substance such as contact lenses. It can develop at any time after wearing contact lenses. An allergic reaction is thought to be one of the causes of GPC. Some individuals are allergic to either their contact lenses or the chemicals used to clean them. An allergic reaction between the skin of the eyelid and the contact lenses or chemicals may be a cause. Other causes of GPC may include repetitive rubbing of the eyes, eye implants, and/or sutures in the eyes from a previous eye surgery. The symptoms may include watery eyes, redness, burning, itching, and/or pain. Treatment includes changing one’s contact lens regularly and limiting the time of wearing them to a few hours per day. Disposable contact lenses may be of some benefit as well. In more severe cases, the individual should stop using contact lenses altogether.
The board certified allergy specialist physicians at Black and Kletz Allergy have over 50 years of experience in diagnosing and treating all types of eye conditions whether allergic or infectious. We treat both pediatric and adult patients. Black & Kletz Allergy has 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. To schedule an appointment, please call any of our offices or you may click Request an Appointment and we will respond within 24 hours by the next business day. We have been servicing the greater Washington, DC metropolitan area for many decades and we look forward to providing you with the utmost state-of-the-art allergy care in a welcoming and pleasant environment.
In the Washington, DC, Northern Virginia, and Maryland metropolitan area, tree pollen usually begins to pollinate in mid-February. The pollination is usually dependent upon the weather such that towards the end of Winter, when it first becomes warm outside, pollen begins to be released from the trees. Depending on the temperatures, tree pollination can occur as early as early February or as late as early March. When the trees produce their pollen, allergy sufferers are usually the first to know because they typically will develop symptoms of hay fever (i.e., allergic rhinitis) and/or asthma. As we approach Spring (late March), the tree pollen counts rise and so do the symptoms of individuals with tree pollen allergies. In the Washington, DC metro area, tree pollen counts continue to rise and generally peak in April. This milestone is usually recognized by millions of people as they become aware that all of the cars appear “yellow” in color. The yellowish color of the cars is due to the yellow-colored tree pollen falling on and sticking to the numerous motor vehicles that dominate the DC metro area. The tree pollen count will then decrease and usually end by the end of May. Note that as tree pollination decreases, grass pollination begins. Grass pollen is also a major allergen in many allergic individuals.
It is noteworthy to mention that most people in the DC metro area, who are unfamiliar with allergies, think that it is the cherry trees that are causing their allergy symptoms. This fallacy is believed and propagated because people with tree pollen allergies usually feel miserable around the same time that the cherry trees in the Washington, DC area begin to bloom. What most people do not realize is that in general, flowering trees and plants do not cause allergic symptoms for the most part. The reason for this is that individuals who suffer allergy symptoms from tree pollen need to breathe in the pollen in order to develop the typical symptoms of hay fever. The pollen of flowering trees and plants is heavy compared with non-flowering trees. The lighter pollen found on non-flowering trees (e.g., birch, cedar, elm, ash, beech, hickory, maple, oak) are wind-dispersed. These pollens will travel in the air for hundreds of miles sometimes in order to settle on other trees which will cause the trees to continue to reproduce. With flowering trees and plants, since the pollen is heavy, wind will not suffice to spread the pollen. In order to reproduce, the pollen on flowering trees and plants require the aid of bees, hummingbirds, moths, butterflies, beetles, etc. to land on the flowers to help with the cross-pollination. For example, a bee will be attracted to a flower and as it lands on the flower, the tree pollen sticks to its abdomen. When the bee then lands on another flowering tree or plant, the pollen is transferred to that flower and cross-pollination occurs which allows further reproduction. An easy way to think of it is as follows: It is the pollen of the “ugly” trees that are wind-dispersed and thus cause allergies.
The symptoms that individuals generally experience with tree pollen allergies may include one or more of the following: sneezing, runny nose, nasal congestion, post-nasal drip, itchy nose, itchy eyes, watery eyes, redness of the eyes, itchy throat, itchy ears, clogged ears, sinus pressure, headaches, snoring, fatigue, wheezing, chest tightness, coughing, shortness of breath.
The diagnosis of tree pollen allergies can be made by seeing a board certified allergist such as the ones at Black & Kletz Allergy. A comprehensive history and physical examination are obtained and then usually allergy testing is performed in order to identify an allergy to a specific allergen (e.g., tree pollen). Allergy tests can be done by either skin testing or blood testing, although skin testing is generally the preferred method.
Once an individual is diagnosed with tree pollen allergies, avoidance measures are discussed, although the goal of allergy treatment is to allow the person to enjoy their hobbies (e.g., gardening, golf, hiking) rather than being restricted to being indoors for 3 months every Spring. In addition, there are numerous medications that an allergist can prescribe in order to help alleviate the unwanted allergy symptoms of the allergy sufferer. These medications come in the forms of tablets, syrups, nasal sprays, eye drops, lung inhalers, and injections. If an individual has additional allergies such as grasses, weeds, dust mites, molds, pets, etc., then allergy shots (i.e., allergy injections, allergy immunotherapy, allergy desensitization, allergy hyposensitization) may be recommended. Allergy shots are effective in 80-85% of the patients that take them. They have been used in the United States for more than 100 years. They are given to little children as well as older adults. The average person is on allergy shots for 3-5 years.
If you think that you may have tree pollen allergies, or any other type of allergy, the board certified allergists at Black & Kletz Allergy would be happy to help you. We have 3 convenient offices in the DC metro area with office locations in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our office offer on-site parking. Our Washington, DC and McLean, VA locations are Metro accessible. There is also a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. Please call us for an appointment. Alternatively, you can click Request an Appointment and we will respond to your request within 24 hours by the next business day. The allergists at Black & Kletz Allergy have been treating both adults and children in the Washington, DC metropolitan area for allergies, asthma, sinus disease, and immunologic disorders for more than 50 years. We strive to provide top-of-the-line allergy relief in a caring and professional environment.
Acute sinusitis may also be referred to as acute rhinosinusitis or more commonly as a classic “sinus infection.” By definition, the symptoms of acute sinusitis will last less than 4 weeks in duration, rather than the 12 weeks or more necessary to characterize a sinus infection as chronic sinusitis or a chronic sinus infection. Of note, some physicians classify a sinus infection that lasts from 4 to 12 weeks as subacute sinusitis. The term recurrent sinusitis refers to repeated acute sinus infections but can easily be confused with a chronic sinus infection. This distinction is particularly important to differentiate as an allergist because the workup and treatment of recurrent sinus infections is quite different than the workup and treatment of a chronic sinus infection.
Acute sinusitis is most commonly caused by the “common cold” or another type of virus. Most of the time, the acute sinusitis is self-limited and resolves without treatment in 7-10 days. Approximately 1-2% of sinusitis caused by viruses will result in a subsequent bacterial sinus infection. Rarely, a fungus may be the cause of a sinus infection. Other factors that predispose an individual to develop acute sinusitis include allergic rhinitis (i.e., hay fever), a deviated nasal septum, nasal polyps, a fixed nasal obstruction (e.g., tumor, foreign body), cystic fibrosis, immunological deficiencies (e.g., HIV/AIDS, diabetes mellitus, common variable immunodeficiency), immunosuppressant medications (i.e., medications that suppress the immune system such as azathioprine, cyclosporine, corticosteroids, and many “biological” medications such as adalimumab, secukinumab, abatacept, infliximab, etanercept), dental and/or periodontal infections, and chemical irritation (e.g., cigarette smoke, chemical fumes).
The symptoms of acute sinusitis typically involves one or more of the following:
Nasal congestion
Discolored nasal discharge (e.g., yellow, green, brown discharge)
Post-nasal drip
Sore throat
Sinus pressure
Sinus headaches
Bad breath
Fatigue
Fever
Radiation of pain to the teeth and/or ears
Clogged ears
Cough
Complications from acute sinusitis is uncommon nowadays in the era of better diagnostic techniques and antibiotics, however, a few complications can still occur and are as follows:
Meningitis
Osteomyelitis (i.e., bone infection)
Cellulitis (i.e., skin infection)
Chronic sinusitis
Visual disturbances (if the infection spreads to one’s eye)
Decreased or loss of sense of smell
The diagnosis of acute sinusitis is usually a clinical one. The history that the patient describes along with certain findings on physical examination in most cases is usually enough to diagnose the individual. Other methods that are utilized by physicians may include allergy testing, rhinolaryngoscopy (i.e., small endoscopic instrument used to obtain direct visual inspection of the nose, throat, and vocal cords), radiological studies (e.g., CT scan, MRI), and/or nasal cultures.
The treatment of acute sinusitis most of the time requires no treatment at all. This is so because most cases of acute sinusitis are caused by a virus which usually resolves on its own. In patients who have a bacterial sinus infection or who develop a secondary bacterial infection, antibiotics may be needed to eradicate the infection, particularly if the symptoms persist, worsen, or are severe. In addition, supplemental use of saline nasal irrigation, nasal corticosteroids, decongestants, and/or over-the-counter analgesics are quite helpful in many cases of acute sinusitis to reduce symptoms. It is also recommended to stay hydrated by drinking water.
The prevention of episodes of acute sinusitis can be facilitated by seeing a board certified allergist, like the ones at Black & Kletz Allergy. The allergy specialist will perform a comprehensive history and physical and if necessary will do allergy skin testing to identify if and what allergens are allergenic to the patient. Depending on the frequency of episodes of acute sinusitis and/or allergy symptoms, the allergy doctor will prescribe different medications (i.e., antihistamines, decongestants, nasal sprays, eye drops) used to alleviate the individual’s allergy symptoms. He may also recommend allergy shots (i.e., allergy injections, allergy immunotherapy, allergy hyposensitization) which is effective in 80-85% of patients receiving allergy shots. The allergists at Black & Kletz Allergy treat both adults and pediatric patients and have been doing so in the Washington, DC, Northern Virginia, and Maryland metropolitan area for more than one half a century.
Black & Kletz Allergy has 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. The allergists at Black & Kletz Allergy are extremely knowledgeable regarding the diagnosis and treatment of acute sinusitis and other sinus diseases. In addition, we treat patients with environmental allergies, medication allergies, insect sting allergies, food allergies, eczema, asthma, hives, swelling episodes, generalized itching, contact dermatitis, eosinophilic esophagitis, and immune disorders. To schedule an appointment, please call any of our offices or you may click Request an Appointment and we will respond within 24 hours by the next business day. We have been servicing the greater Washington, DC area for many years and we look forward to providing you with excellent state-of-the-art allergy care in a friendly and professional environment.




 Proton pump inhibitors (PPIs) are a group of medications commonly used to treat symptoms caused by excessive stomach acid. The most common PPIs available in the U.S. are Nexium (i.e., esomeprazole), Protonix (i.e., pantoprazole), Prilosec (i.e., omeprazole), Prevacid (i.e., lansoprazole), Aciphex (i.e., rabeprazole), and Dexilant (i.e., dexlansoprazole). These medications act by reducing the amount of acid secretion produced by the parietal cells in the lining of the stomach. In addition to lifestyle and dietary modifications, they are usually the first line medications prescribed to treat common conditions such as gastroesophageal reflux disease (GERD),
Proton pump inhibitors (PPIs) are a group of medications commonly used to treat symptoms caused by excessive stomach acid. The most common PPIs available in the U.S. are Nexium (i.e., esomeprazole), Protonix (i.e., pantoprazole), Prilosec (i.e., omeprazole), Prevacid (i.e., lansoprazole), Aciphex (i.e., rabeprazole), and Dexilant (i.e., dexlansoprazole). These medications act by reducing the amount of acid secretion produced by the parietal cells in the lining of the stomach. In addition to lifestyle and dietary modifications, they are usually the first line medications prescribed to treat common conditions such as gastroesophageal reflux disease (GERD),  Air pollution is a major problem in many parts of the world particularly in major cities in the U.S. including
Air pollution is a major problem in many parts of the world particularly in major cities in the U.S. including 
 Coughing is a protective “reflex” given to us by nature as part of our body’s vital defense mechanisms. It forcibly expels harmful bacteria, viruses, foreign objects, and excessive mucus from the respiratory tract protecting our lungs from irritation, inflammation, and infections.
Coughing is a protective “reflex” given to us by nature as part of our body’s vital defense mechanisms. It forcibly expels harmful bacteria, viruses, foreign objects, and excessive mucus from the respiratory tract protecting our lungs from irritation, inflammation, and infections. Symptoms such as nasal congestion, clear runny nose, and itchy throat are most commonly due to sensitivity to common “allergens” in the environment (e.g., pollens, dust mites, mold spores, animals). Our immune system mistakes them as potentially harmful and thus mounts a defensive attack on these substances when it encounters them. During this process, there is a release of chemical substances (e.g., histamine, prostaglandins, leukotrienes) into the tissues inside the nose and eyes and these chemicals are responsible for the symptoms of allergies.
Symptoms such as nasal congestion, clear runny nose, and itchy throat are most commonly due to sensitivity to common “allergens” in the environment (e.g., pollens, dust mites, mold spores, animals). Our immune system mistakes them as potentially harmful and thus mounts a defensive attack on these substances when it encounters them. During this process, there is a release of chemical substances (e.g., histamine, prostaglandins, leukotrienes) into the tissues inside the nose and eyes and these chemicals are responsible for the symptoms of allergies. Does eating local honey help treat allergies? This question has been asked for decades. Many individuals swear that consuming local honey does help alleviate their seasonal allergy symptoms known as
Does eating local honey help treat allergies? This question has been asked for decades. Many individuals swear that consuming local honey does help alleviate their seasonal allergy symptoms known as  Eczema (i.e., atopic dermatitis) is a genetically determined condition which causes long term inflammation of the skin which may result in itching, thickening, redness, and occasionally ulcerations of the skin. A similar appearance can sometimes be seen in other chronic skin conditions.
Eczema (i.e., atopic dermatitis) is a genetically determined condition which causes long term inflammation of the skin which may result in itching, thickening, redness, and occasionally ulcerations of the skin. A similar appearance can sometimes be seen in other chronic skin conditions. As we enter the Spring season in the
As we enter the Spring season in the  The most common cause in the Washington, DC, Northern Virginia, and Maryland metropolitan area for itchy, red eyes in the Spring and Fall high pollen seasons is inflammation of the thin membrane covering the eyeballs (i.e., conjunctivae). This inflammation is triggered by allergen exposure to susceptible individuals. However, inflammation to the conjunctivae can also be caused by infections by microorganisms such as viruses, bacteria, and rarely fungi and parasites.
The most common cause in the Washington, DC, Northern Virginia, and Maryland metropolitan area for itchy, red eyes in the Spring and Fall high pollen seasons is inflammation of the thin membrane covering the eyeballs (i.e., conjunctivae). This inflammation is triggered by allergen exposure to susceptible individuals. However, inflammation to the conjunctivae can also be caused by infections by microorganisms such as viruses, bacteria, and rarely fungi and parasites.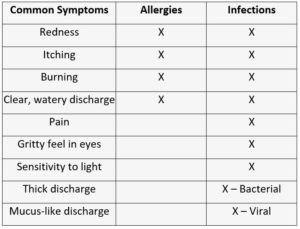
 In the
In the  Acute sinusitis may also be referred to as acute rhinosinusitis or more commonly as a classic “sinus infection.” By definition, the symptoms of acute sinusitis will last less than 4 weeks in duration, rather than the 12 weeks or more necessary to characterize a sinus infection as chronic sinusitis or a chronic sinus infection. Of note, some physicians classify a sinus infection that lasts from 4 to 12 weeks as subacute sinusitis. The term recurrent sinusitis refers to repeated acute sinus infections but can easily be confused with a chronic sinus infection. This distinction is particularly important to differentiate as an allergist because the workup and treatment of recurrent sinus infections is quite different than the workup and treatment of a chronic sinus infection.
Acute sinusitis may also be referred to as acute rhinosinusitis or more commonly as a classic “sinus infection.” By definition, the symptoms of acute sinusitis will last less than 4 weeks in duration, rather than the 12 weeks or more necessary to characterize a sinus infection as chronic sinusitis or a chronic sinus infection. Of note, some physicians classify a sinus infection that lasts from 4 to 12 weeks as subacute sinusitis. The term recurrent sinusitis refers to repeated acute sinus infections but can easily be confused with a chronic sinus infection. This distinction is particularly important to differentiate as an allergist because the workup and treatment of recurrent sinus infections is quite different than the workup and treatment of a chronic sinus infection.








