
 Winter is around the corner and so are the annoying allergy symptoms that some individuals experience during this time of the year. Classically, in the Washington, DC, Northern VA, and Maryland metropolitan area, when people think of hay fever (i.e., allergic rhinitis), they think of allergy symptoms that occur in the Spring and/or Fall. The allergens that cause these bothersome symptoms in the Spring and Fall are primarily pollens. Tree and grass pollens generally cause allergy symptoms in the Spring, whereas weed pollens are commonly responsible for allergy symptoms in the Fall. It should be noted that mold is also a very common allergen which often increases in the Fall, particularly around decomposing fallen leaves.
Winter is around the corner and so are the annoying allergy symptoms that some individuals experience during this time of the year. Classically, in the Washington, DC, Northern VA, and Maryland metropolitan area, when people think of hay fever (i.e., allergic rhinitis), they think of allergy symptoms that occur in the Spring and/or Fall. The allergens that cause these bothersome symptoms in the Spring and Fall are primarily pollens. Tree and grass pollens generally cause allergy symptoms in the Spring, whereas weed pollens are commonly responsible for allergy symptoms in the Fall. It should be noted that mold is also a very common allergen which often increases in the Fall, particularly around decomposing fallen leaves.If pollens are generally a problem in the Spring and Fall, why do so many people experience allergy symptoms in the Winter? What allergens are causing individuals to feel so lousy during the coldest time of the year? The answer is not a simple one. There are many allergens that may wreak havoc on sensitive allergic individuals during the Winter. The most common allergens responsible for Winter allergies may include dust mites, molds, pets, and/or cockroaches.
As far a dust mites are concerned, in the Washington, DC metro area, the 2 common species of dust mites are Dermatophagoides fariniae (i.e., American dust mite) and Dermatophagoides pteronyssinus (i.e., European dust mite). Both of these species are quite allergenic. In fact, it is the fecal particles and exoskeleton that are the allergenic components of the dust mites. Dust mites are usually found indoors in places such as in bedding (i.e., pillows, mattresses, box springs), carpeting, and upholstered furniture. They are microscopic in nature and look similar to cockroaches except they cannot be seen with the naked eye. They are approximately 0.25 mm. in length. Dust mites survive by eating the dead skin that habitually sloughs off of humans each night, hence they are commonly found in bedding. Dust mites flourish in high humidity, warm, moist climates. They do not survive if the temperature is over 130° F or when the altitude is greater than 1 mile (5,280 feet). Dust mites are known to be a common cause of allergic rhinitis, allergic conjunctivitis (i.e., eye allergies) and asthma in many sensitive individuals. Dust mites can be killed with the application of miticide products, however these products have not been shown to be that efficacious. Encasing one’s pillows, mattresses, and box springs in allergy-proof encasings are a fairly effective way to minimize one’s exposure to dust mites.
In the Winter, many people close up their homes by keeping the windows closed and recirculating the air. As a result, indoor allergens such as dust mites, molds, pet dander, and cockroach become trapped in the home causing an individual to breathe in more allergen than during other times of the year when the windows tend to be open more often.
Cockroach allergy is common particularly in major cities such as Washington, DC and New York City. They are potent allergens. Many apartments, condos, homes, restaurants, and public buildings in inner cities are infested with cockroaches, even though they may not be visible during the day to most people. It is important to make sure that traces of food are not left on countertops and floors, as this entices cockroaches. There is also a strong association between cockroach allergy and childhood asthma in inner city populations. Cockroach allergies may cause allergic rhinitis, allergic conjunctivitis, and/or asthma symptoms in sensitive allergic individuals.
Pet allergens from the dander and saliva tend to be worse in the Winter due to the closed up nature of a typical house. People who are allergic to pets but refuse to give them up should at least not allow the pet to venture into their bedroom, if at all possible. This will give the individual a “pet-free” zone in the bedroom, where people tend to spend the most time.
Mold allergy is also prevalent during the Winters in the Washington, DC metropolitan area. Washington, DC was built on a swamp and as a result the abundance of mold is commonplace. Similar to dust mite, cockroach, and pet allergies, mold is an indoor allergen, however, unlike dust mite, cockroach, and pet allergies, mold is also found outdoors. This double whammy makes mold allergy a unique allergen in that it affects people both indoors and outdoors. It is recommended that people keep the relative humidity in their homes to be below 33%.
In a perfect world, avoidance of the offending allergen is obviously the best option to prevent environmental allergies. In reality however, it is very difficult, if not impossible, to avoid contact with some of these ubiquitous allergens. So if one is unable to avoid these allergens, there are numerous medications that can be used by allergy doctors to treat dust mite, mold, pet, and cockroach allergies. In addition to various antihistamines, decongestants, nasal sprays, and allergy eye drops, allergy shots (i.e., allergy injections, allergy immunotherapy, allergy desensitization) are a very effective tool that board certified allergy specialists use to treat individuals with these allergies, as well as pollen allergies. Allergy injections are effective in 80-85% of the patients. Allergy shots have been used in the U.S. to treat allergies and asthma for over 100 years. The average length of treatment is 3-5 years.
The board certified allergy specialists of Black & Kletz Allergy have been treating pediatric and adult patients with allergies and asthma for over 5 decades. Black & Kletz Allergy has 3 offices in the Washington, DC, Northern Virginia, and Maryland metropolitan area. We have convenient offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. Our offices in Washington, DC and McLean, VA are Metro accessible with free shuttle service between the Spring Hill metro station and our McLean office. All 3 locations offer on-site parking. To make an appointment, please call us, or alternatively you can click Request an Appointment and we will respond within 24 hours on the next business day. The allergists at Black & Kletz Allergy strive to manage your allergy and asthma to your utmost satisfaction in a professional caring atmosphere.
 Much of the information from the past decade regarding when to introduce peanuts into the diet of infants has been reviewed recently and subsequently revised. Research over the past 9 years shows that early introduction and regular consumption of peanuts decreases the risk of developing a peanut allergy. It is no longer recommended that parents delay the introduction of peanuts in most children, as delay beyond 12 months may actually increase the risk of peanut allergy.
Much of the information from the past decade regarding when to introduce peanuts into the diet of infants has been reviewed recently and subsequently revised. Research over the past 9 years shows that early introduction and regular consumption of peanuts decreases the risk of developing a peanut allergy. It is no longer recommended that parents delay the introduction of peanuts in most children, as delay beyond 12 months may actually increase the risk of peanut allergy.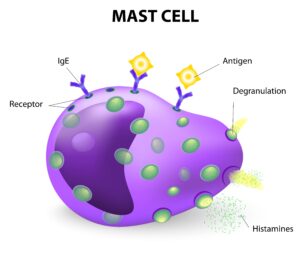 Mast cells are types of white blood cells that generally are found in the connective tissues. There are granules inside the mast cells that contain chemical mediators such as histamine, heparin, tryptase, prostaglandins, leukotrienes, serotonin, and cytokines. Many of these mediators are inflammatory in nature. In addition, mast cells have the allergy antibody, known as IgE, attached to their surfaces. Mast cells play an important role in initiating and promoting immune responses to pathogens (i.e., bacteria, viruses) and toxins (i.e., mold, flying insect stings) by releasing these chemical mediators Mast cells are also responsible for immediate allergic reactions. In an allergic reaction, the IgE on the surface of the mast cells bind to the proteins (i.e., allergens) that cause allergies. The mast cell is now activated, which causes the granules and their contents to be extruded from the mast cells into the tissues in a process called degranulation. As a result, the chemical mediators, which include histamine and chemicals that cause inflammation, are released into the tissues. These chemicals cause the typical symptoms that are generally associated with allergies such as
Mast cells are types of white blood cells that generally are found in the connective tissues. There are granules inside the mast cells that contain chemical mediators such as histamine, heparin, tryptase, prostaglandins, leukotrienes, serotonin, and cytokines. Many of these mediators are inflammatory in nature. In addition, mast cells have the allergy antibody, known as IgE, attached to their surfaces. Mast cells play an important role in initiating and promoting immune responses to pathogens (i.e., bacteria, viruses) and toxins (i.e., mold, flying insect stings) by releasing these chemical mediators Mast cells are also responsible for immediate allergic reactions. In an allergic reaction, the IgE on the surface of the mast cells bind to the proteins (i.e., allergens) that cause allergies. The mast cell is now activated, which causes the granules and their contents to be extruded from the mast cells into the tissues in a process called degranulation. As a result, the chemical mediators, which include histamine and chemicals that cause inflammation, are released into the tissues. These chemicals cause the typical symptoms that are generally associated with allergies such as  It is that time of the year again. Soon you will be seeing children (and some adults) trick or treating in your neighborhood searching for candy. For children, Halloween is a time to be with their friends, eat a lot of candy, and dress in scary costumes. For millions of parents however, Halloween can also be scary, but for a different reason: Their children have food allergies. According to Food Allergy Research & Education (FARE), approximately 6 million or 1 in 13 children in the U.S. have food allergies. This is about 8% of the U.S. pediatric population which is equivalent to about 2 children per classroom. In addition, more than 26 million adults also have food allergies. Together, there are about 32 million individuals with food allergies in the U.S. which is approximately 10% of the population. What is even more frightening is that the food allergy prevalence among children has increased dramatically within the last 30 years.
It is that time of the year again. Soon you will be seeing children (and some adults) trick or treating in your neighborhood searching for candy. For children, Halloween is a time to be with their friends, eat a lot of candy, and dress in scary costumes. For millions of parents however, Halloween can also be scary, but for a different reason: Their children have food allergies. According to Food Allergy Research & Education (FARE), approximately 6 million or 1 in 13 children in the U.S. have food allergies. This is about 8% of the U.S. pediatric population which is equivalent to about 2 children per classroom. In addition, more than 26 million adults also have food allergies. Together, there are about 32 million individuals with food allergies in the U.S. which is approximately 10% of the population. What is even more frightening is that the food allergy prevalence among children has increased dramatically within the last 30 years. Immunizations are one of the most effective and safe ways of preventing or reducing the risk of serious illness from various infections. Vaccinations also prevent infections from spreading from one individual to another, thus protecting the health and well-being of the general population. One should always check with one’s primary care provider before getting a vaccine. The CDC recommends vaccines for adults based on a variety of factors which may include age, travel destinations, sexual activity, health history, occupation, lifestyle, and previous vaccinations. The CDC currently recommends the following immunizations:
Immunizations are one of the most effective and safe ways of preventing or reducing the risk of serious illness from various infections. Vaccinations also prevent infections from spreading from one individual to another, thus protecting the health and well-being of the general population. One should always check with one’s primary care provider before getting a vaccine. The CDC recommends vaccines for adults based on a variety of factors which may include age, travel destinations, sexual activity, health history, occupation, lifestyle, and previous vaccinations. The CDC currently recommends the following immunizations: In children with milk allergy, the immune system falsely identifies the protein in the milk as potentially dangerous, and as a result, mounts a defensive attack. The “pre-formed” milk specific antibodies (i.e., immunoglobulin E or IgE) react with the protein in the milk (i.e., antigen), causing release of chemical substances (e.g., histamine, leukotrienes, prostaglandins) into the tissues. These chemical substances are what causes the symptoms of allergic reactions. Cow’s milk is the most common cause of milk allergy although milk from sheep and goats can also cause allergic reactions in certain sensitized children. Children are more likely to have a milk allergy if there is a history of a food allergy in other family members.
In children with milk allergy, the immune system falsely identifies the protein in the milk as potentially dangerous, and as a result, mounts a defensive attack. The “pre-formed” milk specific antibodies (i.e., immunoglobulin E or IgE) react with the protein in the milk (i.e., antigen), causing release of chemical substances (e.g., histamine, leukotrienes, prostaglandins) into the tissues. These chemical substances are what causes the symptoms of allergic reactions. Cow’s milk is the most common cause of milk allergy although milk from sheep and goats can also cause allergic reactions in certain sensitized children. Children are more likely to have a milk allergy if there is a history of a food allergy in other family members. Generalized itching (i.e., generalized pruritus) is a condition which can be quite annoying. It is when an individual has diffuse itching of the body usually without an associated rash. Approximately 20-25% of the general population experiences generalized pruritus at least one time in their life. The itching may be intermittent or it may be chronic in nature. “Acute” itching is when the itching has been present for less than 6 weeks. “Chronic” itching is defined by having it for 6 or more weeks. The itching may last for years in certain individuals. The severity of the itching may vary from very mild to very severe where it can interfere with one’s quality of life. If the itching becomes chronic, it is important to see a
Generalized itching (i.e., generalized pruritus) is a condition which can be quite annoying. It is when an individual has diffuse itching of the body usually without an associated rash. Approximately 20-25% of the general population experiences generalized pruritus at least one time in their life. The itching may be intermittent or it may be chronic in nature. “Acute” itching is when the itching has been present for less than 6 weeks. “Chronic” itching is defined by having it for 6 or more weeks. The itching may last for years in certain individuals. The severity of the itching may vary from very mild to very severe where it can interfere with one’s quality of life. If the itching becomes chronic, it is important to see a  Anaphylaxis is an acute, severe, and life-threatening allergic reaction. The most common triggers for anaphylaxis include allergenic foods, medications, and insect stings. Symptoms usually begin within a few minutes of exposure of the triggering agents. Initially, the symptoms characteristically involve the skin which typically causes itching and hives followed by swelling of the soft tissues. Unless treated, the reaction may rapidly progress and may involve other organ systems (e.g., respiratory, gastrointestinal, cardiovascular) resulting in symptoms such as shortness of breath, wheezing, coughing, nausea, vomiting, abdominal pain, dizziness, drop in blood pressure, and/or loss of consciousness.
Anaphylaxis is an acute, severe, and life-threatening allergic reaction. The most common triggers for anaphylaxis include allergenic foods, medications, and insect stings. Symptoms usually begin within a few minutes of exposure of the triggering agents. Initially, the symptoms characteristically involve the skin which typically causes itching and hives followed by swelling of the soft tissues. Unless treated, the reaction may rapidly progress and may involve other organ systems (e.g., respiratory, gastrointestinal, cardiovascular) resulting in symptoms such as shortness of breath, wheezing, coughing, nausea, vomiting, abdominal pain, dizziness, drop in blood pressure, and/or loss of consciousness. As the Summer marches on and we are now in the month of August, many allergy sufferers are about to get ready for another foe, namely ragweed. Usually about August 15th of every year, ragweed pollen begins to blanket the
As the Summer marches on and we are now in the month of August, many allergy sufferers are about to get ready for another foe, namely ragweed. Usually about August 15th of every year, ragweed pollen begins to blanket the  Contact dermatitis
Contact dermatitis Now that it is Summer, mosquitoes are becoming more prevalent in the Washington, DC, Northern Virginia, and Maryland region. Mosquitoes are flying insects that tend to be more widespread where there is standing water. They are more active early in the morning and early in the evening. Female mosquitoes typically lay their eggs in stagnant water. Only the female mosquito bites and feeds on human blood, as they need this blood in order to produce their eggs. Male mosquitoes, on the other hand, feed on water and nectar. Mosquitoes are considered pests and they are a nuisance to almost everyone who comes in contact with these annoying insects. When a person is bitten, the mosquito injects its saliva into the skin which contains proteins that prevent the human blood from clotting. This allows the blood to be transferred to the mosquito’s mouth without clotting. For the most part, mosquitoes bite people and animals without any symptoms or only very mild local symptoms. For many others however, a mosquito bite can cause a great deal of misery, mostly consisting of irritation, itching, redness, and/or swelling at the site of the bite. In very sensitive individuals, the swelling and redness can become quite large. Occasionally this redness and swelling is accompanied by bruising and/or blisters.
Now that it is Summer, mosquitoes are becoming more prevalent in the Washington, DC, Northern Virginia, and Maryland region. Mosquitoes are flying insects that tend to be more widespread where there is standing water. They are more active early in the morning and early in the evening. Female mosquitoes typically lay their eggs in stagnant water. Only the female mosquito bites and feeds on human blood, as they need this blood in order to produce their eggs. Male mosquitoes, on the other hand, feed on water and nectar. Mosquitoes are considered pests and they are a nuisance to almost everyone who comes in contact with these annoying insects. When a person is bitten, the mosquito injects its saliva into the skin which contains proteins that prevent the human blood from clotting. This allows the blood to be transferred to the mosquito’s mouth without clotting. For the most part, mosquitoes bite people and animals without any symptoms or only very mild local symptoms. For many others however, a mosquito bite can cause a great deal of misery, mostly consisting of irritation, itching, redness, and/or swelling at the site of the bite. In very sensitive individuals, the swelling and redness can become quite large. Occasionally this redness and swelling is accompanied by bruising and/or blisters. Grass pollen allergy is a very common environmental allergy. Grass pollinates in at different time of the year depending on where in the U.S. one is located. In the Northeastern and Mid-Atlantic regions of the U.S., grass pollinates from the Spring through the Summer. In the
Grass pollen allergy is a very common environmental allergy. Grass pollinates in at different time of the year depending on where in the U.S. one is located. In the Northeastern and Mid-Atlantic regions of the U.S., grass pollinates from the Spring through the Summer. In the  In order to understand conjunctivitis, one must first understand a little about the anatomy of the eye as well as a little physiology of the way eyes become lubricated. The conjunctiva is the thin transparent membrane that lines the inside of the eyelids (i.e., palpebral area) and the front of the eyeballs (i.e., bulbar area). The lacrimal glands, which are located in the outer corners of the eyes, secrete tears which lubricate the eyes. These tears then drain into the nose via tear ducts from the inner corners of the eyes. Inflammation of the conjunctival membrane is called conjunctivitis. There are several conditions which cause inflammation of the conjunctiva which are as follows:
In order to understand conjunctivitis, one must first understand a little about the anatomy of the eye as well as a little physiology of the way eyes become lubricated. The conjunctiva is the thin transparent membrane that lines the inside of the eyelids (i.e., palpebral area) and the front of the eyeballs (i.e., bulbar area). The lacrimal glands, which are located in the outer corners of the eyes, secrete tears which lubricate the eyes. These tears then drain into the nose via tear ducts from the inner corners of the eyes. Inflammation of the conjunctival membrane is called conjunctivitis. There are several conditions which cause inflammation of the conjunctiva which are as follows: Summertime in the metropolitan
Summertime in the metropolitan  The symptoms of asthma may include a feeling of chest tightness or heaviness in the chest, wheezing (i.e., high-pitched whistling type of noise during breathing), coughing, and/or shortness of breath/difficulty in breathing. The frequency of these symptoms varies depending on the severity of the asthma. The symptoms can be intermittent or persistent. The severity is also classified as either mild, moderate, or severe. Asthma usually begins in childhood, although it can also be diagnosed for the first time in adulthood. The course of asthma is variable. The symptoms can be mild, moderate, severe, frequent, infrequent, intermittent, and/or persistent at various times throughout one’s life.
The symptoms of asthma may include a feeling of chest tightness or heaviness in the chest, wheezing (i.e., high-pitched whistling type of noise during breathing), coughing, and/or shortness of breath/difficulty in breathing. The frequency of these symptoms varies depending on the severity of the asthma. The symptoms can be intermittent or persistent. The severity is also classified as either mild, moderate, or severe. Asthma usually begins in childhood, although it can also be diagnosed for the first time in adulthood. The course of asthma is variable. The symptoms can be mild, moderate, severe, frequent, infrequent, intermittent, and/or persistent at various times throughout one’s life.








