
 Erythema Multiforme is a type of a rash on the skin, usually triggered by an infection or an adverse effect of a medication. The condition gets its name from the appearance of reddish skin lesions of various forms seen at the same time.
Erythema Multiforme is a type of a rash on the skin, usually triggered by an infection or an adverse effect of a medication. The condition gets its name from the appearance of reddish skin lesions of various forms seen at the same time.
Erythema multiforme affects less than 1% of the population. It is most common in young adults (aged 20 – 40 years) with a modest predominance in males. Some people are genetically predisposed to develop erythema multiforme.
Causes:
Erythema multiforme is an immunological response to either an infection or a medication, manifested on the skin. The most common causative factors are:
- Infections – Herpes simplex virus (most common), mycoplasma, cytomegalovirus, Epstein-Barr virus, influenza virus, coronavirus, etc.
- Medications – Antibiotics (e.g., sulfonamides, tetracyclines, erythromycin), aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., ibuprofen, naproxen), anti-seizure medications, and vaccines.
- Systemic disorders – Inflammatory bowel disease, hepatitis, lymphoma, leukemia, and solid organ tumors.
Diagnosis:
- After exposure to the trigger, there is usually a prodromal period when the individual may experience mild fever, cold like symptoms, sore throat, headache, fatigue, and/or achiness.
- A few days later, the typical skin lesions will erupt. These lesions may be in the form of red papules (i.e., small raised bumps), vesicles (i.e., blisters filled with clear fluid), ulcers (i.e., skin sores), etc.
- Characteristic lesions are ‘bulls-eye’ target lesions with a central dusky area, surrounded by a pale edematous area and a peripheral reddish ring, demarcating it from the surrounding normal skin.
- Atypical lesions are raised with poorly defined borders and/or fewer zones of color variation.
- Several lesions in different developmental stages may be seen at the same time.
- The skin lesions are usually symmetrical, begin at the periphery and spread centrally. The skin lesions usually have a predilection to extensor surfaces (i.e., outer side of the limbs)
- Skin lesions may be very itchy, painful, and/or swollen.
- Confirmation of the diagnosis may require a skin biopsy.
- Tests for infections, especially herpes simplex virus, are needed.
Types:
There are 2 types of erythema multiforme:
Erythema multiforme is not contagious. The lesions, blisters, or rash on the skin cannot spread from person to person. The viruses and other agents that caused the infection, however, can spread from one person to another.
Treatment:
- Most cases of erythema multiforme are mild and self-limiting and usually resolve spontaneously after a few days or weeks.
- Antihistamines and topical corticosteroid medications are helpful in relieving the itching and discomfort associated with more severe skin lesions.
- Antiseptic and local anesthetic mouthwashes may help relieve the pain and irritation associated with mucus membrane lesions inside the mouth.
- Antihistamine or anti-inflammatory eye drops can treat redness, burning, and/or excessive tearing of the eyes.
- Proper care of skin lesions such as avoidance of scratching will help prevent the spread of infections.
- Most severe cases may need a course of systemic corticosteroids such as oral prednisone.
- Recurrent cases are usually treated with 6 months or more of continuous oral antiviral medications such as acyclovir.
Prevention:
- General hand and respiratory hygiene is important in order to reduce the risk of contracting viral and bacterial infections.
- Avoiding medications that had previously caused adverse reactions in the past.
The board certified allergy specialists at Black & Kletz Allergy have 3 locations in the Washington, Northern Virginia, and Maryland metropolitan area. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our offices have on-site parking and the Washington, DC and McLean, VA offices are also Metro accessible. The McLean office has a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. The allergists at Black & Kletz Allergy diagnose and treat both pediatric and adult patients. To make an appointment, please call our office or you may click Request an Appointment and we will respond within 24 hours by the next business day. The allergy doctors at Black & Kletz Allergy have been helping patients with allergic skin rashes, hives (i.e., urticaria), eczema (i.e., atopic dermatitis), as well as other causes of allergies including hay fever (i.e., allergic rhinitis), asthma, sinus disease, food allergies, medication allergies, insect sting allergies, and immunological disorders for more than 50 years. If you suffer from an allergic skin rash or any other type of allergies it is our mission to improve your quality of life by minimizing or preventing your unwanted and annoying allergy symptoms.
 Prurigo nodularis is a chronic inflammatory skin disease where an extremely itchy rash in the form of firm bumps called nodules appears most commonly on the arms, legs, upper back, and/or abdomen. The rash is usually symmetrically distributed on both sides of the body. The itchiness, burning, and stinging sensation associated with prurigo nodularis is so severe that it often interferes with sleep and one’s psychological well-being.
Prurigo nodularis is a chronic inflammatory skin disease where an extremely itchy rash in the form of firm bumps called nodules appears most commonly on the arms, legs, upper back, and/or abdomen. The rash is usually symmetrically distributed on both sides of the body. The itchiness, burning, and stinging sensation associated with prurigo nodularis is so severe that it often interferes with sleep and one’s psychological well-being. Now that Summer is almost here, people tend to spend a lot of time outdoors. Whether it be going to the beach, swimming at the neighborhood pool, playing baseball or softball, having a picnic, fishing, hiking, riding bicycles, gardening, or any other outside activity, people are more likely to be outdoors now than in any other season of the year. Since the general public is outdoors more in the Summers, it should be noted that there are a lot of outdoor allergens that they are being exposed to when outside.
Now that Summer is almost here, people tend to spend a lot of time outdoors. Whether it be going to the beach, swimming at the neighborhood pool, playing baseball or softball, having a picnic, fishing, hiking, riding bicycles, gardening, or any other outside activity, people are more likely to be outdoors now than in any other season of the year. Since the general public is outdoors more in the Summers, it should be noted that there are a lot of outdoor allergens that they are being exposed to when outside. Histamine is a biogenic amine (i.e., an
Histamine is a biogenic amine (i.e., an  Individuals with pollen allergies may be affected throughout the year, depending on where they live or travel. In the
Individuals with pollen allergies may be affected throughout the year, depending on where they live or travel. In the  Although Primatene Mist became available in 1967, the FDA took it off the market in 2011, as it contained propellants called chlorofluorocarbons (CFC’s) which are harmful to the environment as they deplete ozone from the atmosphere. However, Primatene mist was recently reintroduced into the market with a newer propellant called hydrofluoroalkanes (HFA’s), which are environment friendly. Primatene Mist temporarily opens up the airways in the lungs thus offering a very short-term relief from shortness of breath and/or wheezing. It is approved only for individuals with an established prior diagnosis of asthma. It is used for the temporary relief of mild symptoms of intermittent asthma in patients aged 12 years or older and should not be used as a replacement for prescription asthma medications. Primatene Mist can do more harm than good if used for a chronic cough, for instance, without a known cause.
Although Primatene Mist became available in 1967, the FDA took it off the market in 2011, as it contained propellants called chlorofluorocarbons (CFC’s) which are harmful to the environment as they deplete ozone from the atmosphere. However, Primatene mist was recently reintroduced into the market with a newer propellant called hydrofluoroalkanes (HFA’s), which are environment friendly. Primatene Mist temporarily opens up the airways in the lungs thus offering a very short-term relief from shortness of breath and/or wheezing. It is approved only for individuals with an established prior diagnosis of asthma. It is used for the temporary relief of mild symptoms of intermittent asthma in patients aged 12 years or older and should not be used as a replacement for prescription asthma medications. Primatene Mist can do more harm than good if used for a chronic cough, for instance, without a known cause. Pollen food allergy syndrome (PFAS), also known as oral allergy syndrome, is a condition in which there is first a “sensitization” of the immune system to various pollens and subsequent “reactions” when exposed to these pollens. Secondly, there is a similarity of the protein allergens in the pollen and the protein allergens of certain raw or fresh fruits and/or vegetables. The individual’s immune system, which has been previously sensitized to pollen, will also react to the similarly structured proteins in the raw or fresh fruits and/or vegetables. As a result, when a person who has a pollen allergy (usually trees and/or weeds) eats certain raw or fresh fruits and/or vegetables, that individual’s immune system “thinks” that it is being exposed to pollen proteins when in fact it is being exposed to fruit and/or vegetable proteins that have a very similar chemical structure to the pollen proteins. The body in turn reacts to the fresh fruit and/or vegetable proteins in a similar fashion as a typical allergic reaction but is usually more localized to where the food makes direct contact, such as the lips, tongue, palate, ears, gums, and/or throat. Essentially, there is a cross-reaction to the fresh fruit and/or vegetable because that food is mistaken for pollen and thus reacts in a similar way except the reaction is mostly where contact occurs between the food and the mouth. Note that if the fruit or vegetable is cooked, the pollen food allergy reaction does not usually take place because the heating of the fruit and/or vegetable denatures the protein resulting in the immune system not recognizing this denatured protein anymore because the altered structure of the protein does not look like the pollen protein (allergen) anymore.
Pollen food allergy syndrome (PFAS), also known as oral allergy syndrome, is a condition in which there is first a “sensitization” of the immune system to various pollens and subsequent “reactions” when exposed to these pollens. Secondly, there is a similarity of the protein allergens in the pollen and the protein allergens of certain raw or fresh fruits and/or vegetables. The individual’s immune system, which has been previously sensitized to pollen, will also react to the similarly structured proteins in the raw or fresh fruits and/or vegetables. As a result, when a person who has a pollen allergy (usually trees and/or weeds) eats certain raw or fresh fruits and/or vegetables, that individual’s immune system “thinks” that it is being exposed to pollen proteins when in fact it is being exposed to fruit and/or vegetable proteins that have a very similar chemical structure to the pollen proteins. The body in turn reacts to the fresh fruit and/or vegetable proteins in a similar fashion as a typical allergic reaction but is usually more localized to where the food makes direct contact, such as the lips, tongue, palate, ears, gums, and/or throat. Essentially, there is a cross-reaction to the fresh fruit and/or vegetable because that food is mistaken for pollen and thus reacts in a similar way except the reaction is mostly where contact occurs between the food and the mouth. Note that if the fruit or vegetable is cooked, the pollen food allergy reaction does not usually take place because the heating of the fruit and/or vegetable denatures the protein resulting in the immune system not recognizing this denatured protein anymore because the altered structure of the protein does not look like the pollen protein (allergen) anymore. Spring is here! This means that quite a few Washingtonians will be pretty miserable as they will be suffering from
Spring is here! This means that quite a few Washingtonians will be pretty miserable as they will be suffering from  Food protein-induced enterocolitis syndrome (FPIES) is a rare condition that causes gastrointestinal symptoms several hours after consumption of certain foods by an individual who has an intolerance to that food. The prevalence rate in the United States is approximately 0.5%. The most common types of food allergy in children and adults are mediated by an antibody called IgE. Food allergies may result in adverse reactions which in some cases may be very severe and even life-threatening in some that may occur within minutes of ingestion of the offending food. The IgE antibodies are specific to the food that causes the reaction.
Food protein-induced enterocolitis syndrome (FPIES) is a rare condition that causes gastrointestinal symptoms several hours after consumption of certain foods by an individual who has an intolerance to that food. The prevalence rate in the United States is approximately 0.5%. The most common types of food allergy in children and adults are mediated by an antibody called IgE. Food allergies may result in adverse reactions which in some cases may be very severe and even life-threatening in some that may occur within minutes of ingestion of the offending food. The IgE antibodies are specific to the food that causes the reaction.  Some individuals have episodes of swelling or “angioedema” of various tissues that may occur without any known rhyme or reason. They may have 1 episode or they may have multiple or recurrent episodes. Most people with this condition are very surprised and nervous when they notice an area of their body swelling up right in front of their eyes. The swelling can occur on any part of the body or even internally. They may occur by themselves or they may be accompanied with
Some individuals have episodes of swelling or “angioedema” of various tissues that may occur without any known rhyme or reason. They may have 1 episode or they may have multiple or recurrent episodes. Most people with this condition are very surprised and nervous when they notice an area of their body swelling up right in front of their eyes. The swelling can occur on any part of the body or even internally. They may occur by themselves or they may be accompanied with  Four viral infections are surging in the country this year. Three of them are respiratory viruses and one is a gastrointestinal infection. Influenza (“flu”) usually tends to peak in the Winter. The Centers for Disease Control’s (CDC) statistics reveal that more than 30% of the lab tests were positive for the flu in January of this year and the numbers are climbing. 16 deaths related to influenza were reported, bringing the total to 47 deaths so far this season. Respiratory syncytial virus (RSV) numbers peaked in January of this year and are slowly dropping in case numbers.
Four viral infections are surging in the country this year. Three of them are respiratory viruses and one is a gastrointestinal infection. Influenza (“flu”) usually tends to peak in the Winter. The Centers for Disease Control’s (CDC) statistics reveal that more than 30% of the lab tests were positive for the flu in January of this year and the numbers are climbing. 16 deaths related to influenza were reported, bringing the total to 47 deaths so far this season. Respiratory syncytial virus (RSV) numbers peaked in January of this year and are slowly dropping in case numbers.
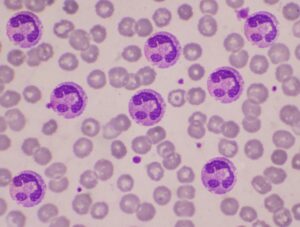 In individuals who are atopic, (i.e., people with a higher incidence of allergic disorders), there will be a higher number of eosinophils in the blood. When there are higher number of eosinophils in the blood than normal, the condition is called eosinophilia. In a disorder named hypereosinophilic syndrome (HES), there are much higher numbers of eosinophils in the blood. Individuals with hypereosinophilic syndrome usually have more than 1,500 eosinophils per microliter in their blood for 6 months or more, and the cause cannot be identified. In addition to being located in the bloodstream, the eosinophils in hypereosinophilic syndrome may also accumulate in various tissues. This excessive eosinophil deposition into the tissues may lead to tissue damage and loss of function.
In individuals who are atopic, (i.e., people with a higher incidence of allergic disorders), there will be a higher number of eosinophils in the blood. When there are higher number of eosinophils in the blood than normal, the condition is called eosinophilia. In a disorder named hypereosinophilic syndrome (HES), there are much higher numbers of eosinophils in the blood. Individuals with hypereosinophilic syndrome usually have more than 1,500 eosinophils per microliter in their blood for 6 months or more, and the cause cannot be identified. In addition to being located in the bloodstream, the eosinophils in hypereosinophilic syndrome may also accumulate in various tissues. This excessive eosinophil deposition into the tissues may lead to tissue damage and loss of function.
 Winter is around the corner and so are the annoying allergy symptoms that some individuals experience during this time of the year. Classically, in the
Winter is around the corner and so are the annoying allergy symptoms that some individuals experience during this time of the year. Classically, in the 








